A paper just published in The Lancet Regional Health — Europe is the strongest evidence yet for an idea that has been quietly reshaping how some surgeons approach ACL surgery: add a small extra ligament reconstruction on the outside of the knee at the same time, and the re-tear rate drops by more than half over the next five years. The signal is biggest in younger patients — the people whose graft-rupture risk is highest to begin with.1
The headline number is striking. At a mean of 5 years, the graft-failure rate was 4.2% with the combined procedure versus 10.3% with a standard isolated ACL reconstruction (adjusted odds ratio 2.54 in favor of the combined approach, p = 0.008). The number needed to treat to prevent one re-tear was 17 overall — and 9 in patients younger than 25. Those are good numbers in a field where most "new" things turn out to add complexity without changing outcomes.1
It is also a study with real limitations a careful patient should know about, and the question of whether your ACL surgery should add this second ligament is more nuanced than the headline suggests. I want to walk through what the trial actually tested, what it found, where the gaps are, and how I am thinking about it in clinic.
What the anterolateral ligament actually is
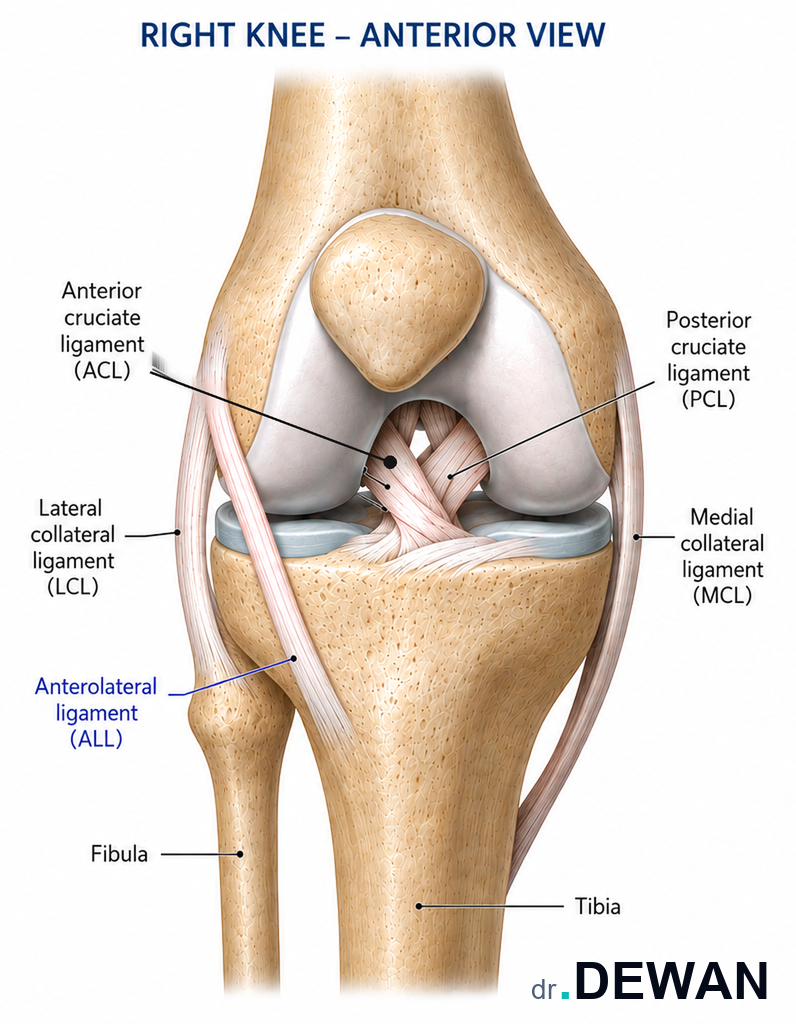
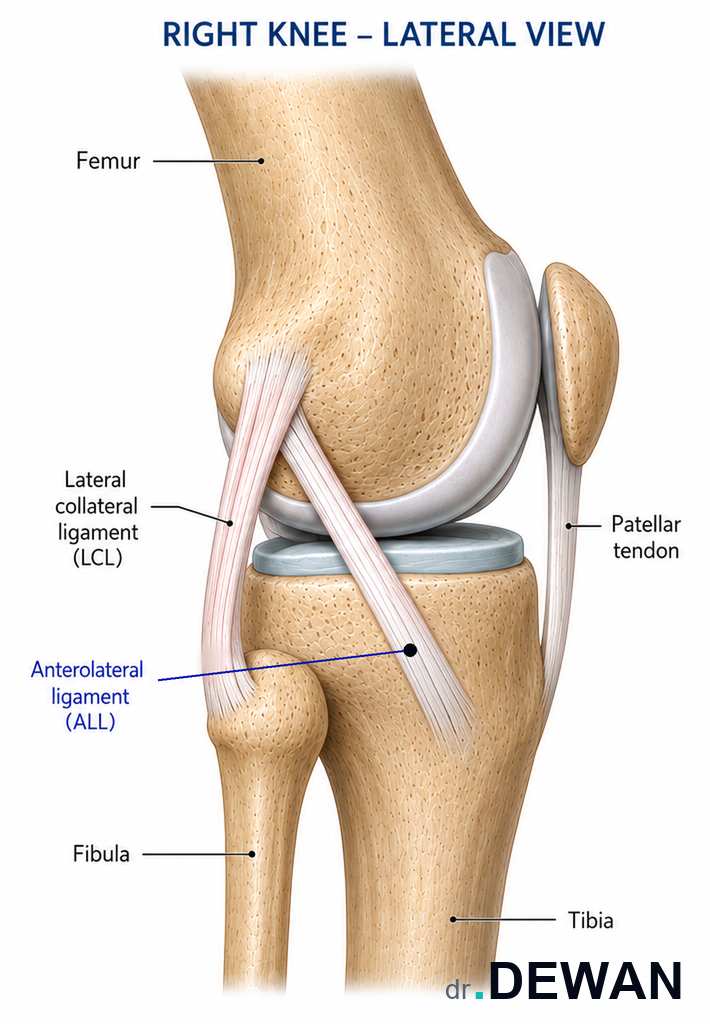
The anterolateral ligament — ALL — is a small ligament on the outer side of the knee, running from the lateral femur (the bump you can feel on the outside of your knee just above the joint) down to a point on the tibia just behind a landmark called Gerdy's tubercle. It is much smaller than the ACL, sits entirely outside the joint, and was only formally described as a distinct anatomic structure in 2013.2
Its job, when it is doing its job, is to help resist rotational instability — the inward-twisting force that produces the famous "pivot shift" that ACL-deficient patients describe as the knee giving way when they plant and cut. The ACL stops the tibia from sliding forward. The ALL — and the related lateral structures — help control how the knee rotates as it bends and straightens.
I should say up front: whether the ALL is truly a discrete ligament — versus a thickening of the joint capsule or the deep iliotibial band — is itself an unsettled anatomic debate. Cadaver studies disagree. Some labs identify a distinct fibrous band in nearly every knee; others find a more variable structure. This matters because the surgical question — "can we strengthen this in a way that protects the ACL graft?" — does not depend on settling the anatomic question. A lateral extra-articular reconstruction can be done either by reconstructing an "ALL" with a tendon graft, or by performing a related, older procedure called a modified Lemaire tenodesis that uses a strip of the iliotibial band to do the same biomechanical job. Most of the recent randomized trials, including the one I'm about to walk through, use the ALL reconstruction technique. The biomechanical principle is the same either way.
What the trial did
The study — Sonnery-Cottet and colleagues at the Santy Orthopedic Center in Lyon, France — was a prospective, single-center, randomized controlled trial.1 The design:
- Patients: 593 adults aged 18–35 (mean age 25, 75% male) with a symptomatic ACL rupture.
- Random allocation: 1:1 to one of two arms.
- Arm A (ACL + ALL): ACL reconstruction using a hamstring tendon autograft, combined with an anterolateral ligament reconstruction.
- Arm B (ACL alone): Standard ACL reconstruction using a bone-patellar tendon-bone (BTB) autograft.
- Primary outcome: Graft failure at 5 years, judged clinically and confirmed on MRI by independent sports-medicine physicians.
- Follow-up: 556 of 593 patients (94%) completed the 5-year visit.
That 94% follow-up is excellent for a 5-year orthopedic trial, and the use of independent MRI-confirmed graft failure as the primary outcome — rather than a softer patient-reported measure — is what gives the result its weight.
What the trial found
Graft failure was less than half as common in the ACL + ALL arm
4.2% (12 of 283) in the combined group vs. 10.3% (28 of 273) in the isolated group. That is a 6.1 percentage-point absolute difference and a 59% relative reduction in graft failure. The adjusted odds ratio was 2.54 (95% confidence interval 1.27 to 5.36, p = 0.008), meaning patients who had an isolated ACL reconstruction had roughly 2.5 times the odds of a re-tear over five years compared with the combined procedure.1
The benefit was concentrated in younger patients
The number needed to treat — how many combined procedures it takes to prevent one re-tear — was 17 overall, but 9 in patients younger than 25. That's a meaningful difference. Treating 9 patients to prevent one re-tear is the kind of margin where surgeons start to take a procedure seriously. Treating 50 or 100 patients to prevent one re-tear is not.
Knee-specific quality-of-life scores were similar between groups
This is the part the headlines don't tell you. The KOOS subscale scores (the standardized knee-injury and osteoarthritis outcome questionnaire) at 5 years were broadly comparable between the two groups. Patients in both arms felt about the same in their day-to-day knee function. The win for the combined procedure was specifically in preventing the catastrophic re-injury — not in making the average knee feel better at 5 years. That distinction matters when you're deciding whether to add a second procedure.
What the trial does well
I want to be fair to the evidence. Several things make this study unusually credible.
It is an actual randomized controlled trial
Most published evidence for adding a lateral procedure to ACL surgery is observational or registry-based, which means it's vulnerable to confounding — surgeons who add the procedure may also operate differently, on different patients, with different rehab. Random allocation handles that. The earlier STABILITY-1 trial (Getgood and the international STABILITY group, AJSM 2020) reported a similar effect with a different lateral technique (modified Lemaire) at 2 years.3 The new Lancet paper extends the randomized evidence to 5 years with a different technique and a different graft pairing — and the direction of the effect is consistent. Two independent RCTs pointing the same way is a stronger evidence package than either one alone.
The primary outcome is hard, not soft
The primary endpoint is graft failure confirmed by MRI and independent physician assessment — not a self-reported pain score that can drift with placebo effects. Hard endpoints are harder to fake, harder to misclassify, and more credible.
The follow-up rate is excellent
94% retention at 5 years is unusual in ACL trials, especially in a young, active population that tends to move around and become hard to find. Losing 6% of patients makes selection bias hard to mount as a serious objection.
The numbers needed to treat are in a clinically meaningful range
An NNT of 9 in patients under 25 is the kind of number that, in another field — cardiology, oncology — would change practice. The orthopedic literature is full of "statistically significant but clinically tiny" findings; this isn't one of them, at least in the young-patient subgroup.
Where the trial has real limitations
This is the part most coverage of the paper skips. A careful read clarifies who the conclusion applies to and where the unanswered questions sit.
The graft type is confounded with the ALL question
This is the single biggest methodological issue, and it's not subtle. The ACL + ALL arm used a hamstring autograft for the ACL. The isolated arm used a bone-patellar tendon-bone (BTB) autograft. Hamstring grafts have a slightly higher published re-tear rate than BTB grafts in some studies, and a slightly lower one in others — but the choice is not neutral. The trial design means we can't fully disentangle "the ALL helped" from "the combination of hamstring + ALL was the right pairing, and BTB alone happened to have a worse year." A cleaner design would have randomized graft type and ALL independently. The authors chose this pairing because it reflects the standard practice at their center — but it limits how cleanly we can attribute the benefit to the ALL itself.
Single center, single surgical team, single high-volume practice
The trial was performed at one institution — the Santy Orthopedic Center, which is among the most experienced ALL-reconstruction practices in the world. Single-center trials generalize less reliably than multicenter trials, and the technical execution of an ALL reconstruction is non-trivial. Whether a surgeon performing one ALL reconstruction a month gets the same result as a surgeon performing five a week is an open question. The Santy group's earlier observational data, the STABILITY-1 international trial, and the new randomized evidence all line up — but the practical effect in an average sports-medicine practice may be smaller than what the trial reports.
The conflicts of interest are substantial
Multiple authors disclose Arthrex consulting fees and research grants. Arthrex manufactures the suspensory-fixation devices commonly used for ALL reconstruction and benefits commercially if more surgeons add lateral procedures. The study itself was not funded by Arthrex (the named funder is a French academic-medical foundation), but the surgical team's financial relationships with the company that makes the implants are real. That doesn't invalidate the data — the outcome assessors were independent — but it should temper the strength with which the findings are presented.1
The young, athletic population is not all ACL patients
The inclusion criteria were 18–35 years old, with symptomatic ACL instability, mostly male, mostly athletic. That is not the average patient walking into an orthopedic office for an ACL consultation. A 42-year-old recreational skier with an ACL tear was not in this trial. Whether a 42-year-old gets the same benefit from adding an ALL reconstruction is an extrapolation, not evidence. The same is true for revision ACL surgery, which the trial did not study.
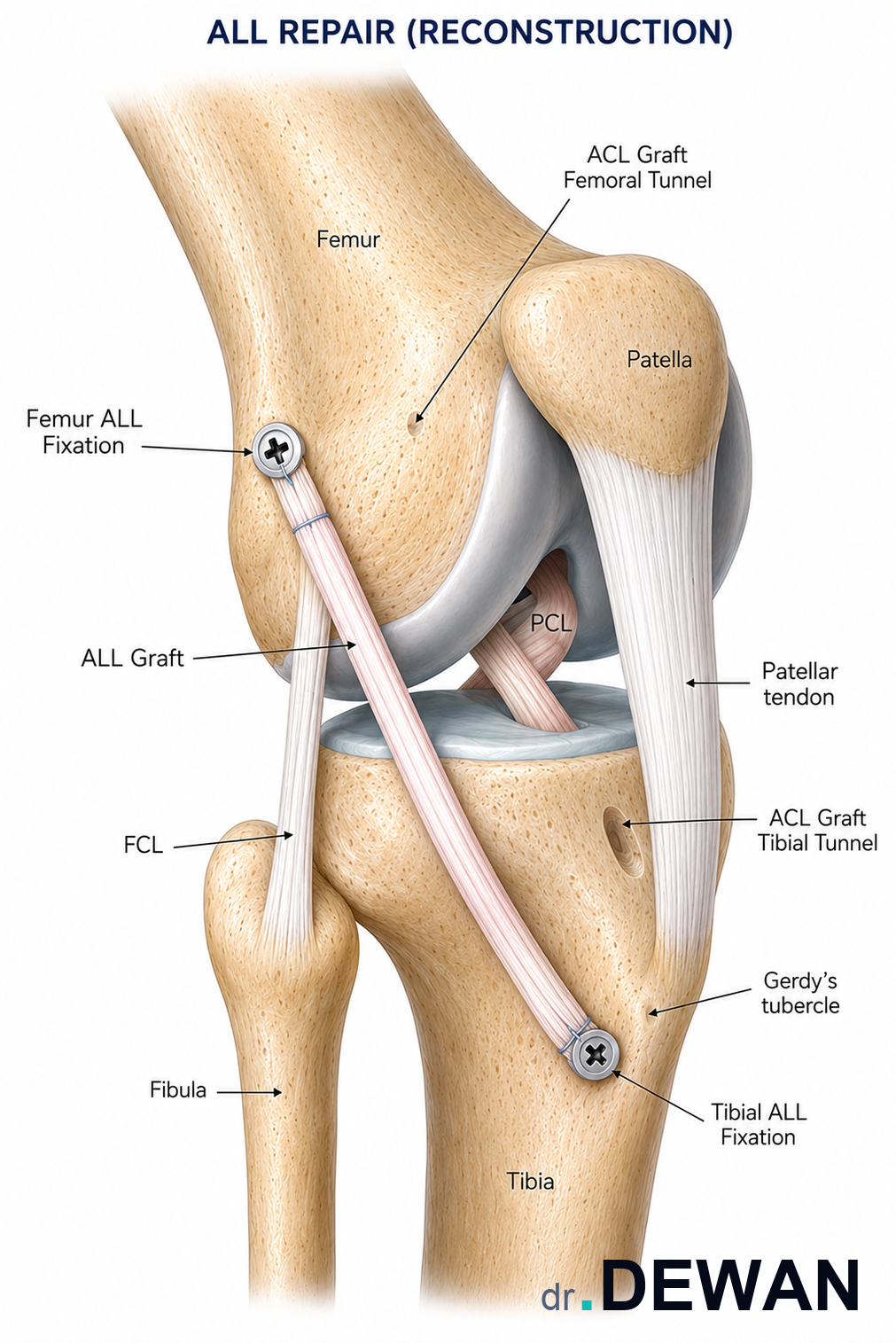
The added procedure has its own costs
Adding an ALL reconstruction means a second incision on the outer side of the knee, two additional bone tunnels (one in the femur, one in the tibia), additional graft material, additional operative time, and a slightly higher rate of lateral-knee numbness from cutaneous nerve irritation. The trial's complication tables don't show a dramatic safety signal, but "no dramatic signal" in a 593-patient trial is not "no risk." Patients should be told this is a real second procedure with its own healing curve, not a free add-on.
"Graft failure" is not the only outcome a patient cares about
The trial's primary endpoint was the failure of the reconstructed ACL graft. That is the right primary endpoint, and re-tearing your ACL is a real disaster — months of additional rehab, a second surgery, often a worse long-term outcome. But patients also care about kneeling comfort, donor-site pain, return to sport at the same level, the feeling of confidence on the field, and long-term osteoarthritis. On most of those, the trial showed comparable results between groups. The case for adding the ALL is specifically about avoiding the catastrophic re-tear — not about a globally better knee at 5 years.
How I am thinking about this in clinic
Evidence like this changes the conversation in clinic without forcing a single answer. When a patient comes in with an ACL tear and is considering reconstruction, here is the sequence I am running through.
How old are you, and how high-risk is your sport?
The biggest signal in the data is in patients younger than 25 — particularly those returning to pivoting sports (soccer, basketball, lacrosse, football). For that patient, the NNT of 9 makes adding a lateral procedure a serious conversation. For a 50-year-old who tore the ACL skiing and wants to return to skiing in a brace, the underlying re-tear risk is much lower to begin with, and adding a second procedure is a less clear win.
Is this a first ACL surgery or a revision?
The published Lancet RCT studied primary reconstructions. For revision ACL surgery — where re-tear rates are already higher and rotational instability is often a contributing cause — there's separate observational evidence (also from the SANTI group) suggesting an even larger benefit from adding a lateral procedure. The published trial does not directly address this, but the biomechanical argument and the observational data both point in the same direction.4
What does the pivot-shift exam look like in the office?
A high-grade pivot shift on physical exam — the knee gives way significantly when the rotational test is performed under anesthesia — is the most direct sign that the rotational stability of the knee is compromised. Patients with a clearly high-grade pivot shift are exactly the patients lateral procedures were designed for, and the conversation about adding one should be more weighted in that direction.
What graft are we using, and why?
The trial paired the ALL reconstruction with a hamstring autograft. If you and I are already planning a BTB or quadriceps-tendon graft (see our graft-choice walkthrough), the calculus shifts. Some surgeons, including me, are not yet convinced that the right move for every BTB ACL reconstruction is to add an ALL on top of it — partly because BTB on its own has good 5-year graft survival in many cohorts, and partly because we don't yet have clean RCT data on that specific pairing.
What is the patient's risk tolerance?
The honest framing of this conversation is: "Adding the lateral procedure adds a second small incision, more time in the operating room, and additional bone tunnels, in exchange for a meaningfully lower 5-year re-tear rate — biggest if you're younger and returning to cutting sports. Here are the numbers; what feels right to you?" Some patients want every reasonable hedge against a re-tear; others want the simpler operation with the established track record. Both are defensible. Evidence-based medicine is not the same as one-size-fits-all medicine.
Where the evidence is currently strongest
Pulling the two randomized trials together — STABILITY-1 with a Lemaire tenodesis at 2 years, and the new Sonnery-Cottet trial with an ALL reconstruction at 5 years — the case for adding a lateral procedure is strongest in:
- Patients under 25
- Returning to high-risk pivoting sports
- With a high-grade pivot shift on exam
- Especially in revision settings or with risk factors for failure (steep posterior tibial slope, generalized ligamentous laxity)
It is less clear for older recreational athletes, sedentary patients, or anyone whose primary concern is donor-site pain rather than re-tear risk.
Bottom line for the layperson
- A new 5-year randomized trial shows that adding a small ligament reconstruction on the outside of the knee — at the same time as your ACL surgery — cuts the re-tear rate from about 10% to about 4% over five years in young, active patients.
- The benefit is biggest in patients under 25 returning to cutting sports. For that group, treating 9 patients with the combined procedure prevents one re-tear.
- The trial's main weakness is that it used different ACL graft types in the two groups, so we can't fully isolate the lateral-ligament effect from the graft-choice effect. A cleaner trial would have separated those.
- Adding the second procedure means another small incision, more operating time, and additional bone tunnels — not a free add-on. The trial did not show a dramatic safety signal, but the trade-off is real.
- If you're young, active, and headed for ACL surgery — ask your surgeon whether adding a lateral procedure (ALL reconstruction or a modified Lemaire tenodesis) is right for your case. Bring your imaging, your sport, and your re-injury concerns to the conversation. Both adding and not adding it can be defensible answers depending on your situation.
If you'd like an independent read on your imaging and your surgical plan, you can request a visit or call the office at (281) 690-4678.
This article reflects Dr. Dewan's reading of the cited evidence at the time of publication. It is educational content, not medical advice. Your specific case may differ — schedule a consultation to discuss your imaging and history.
Sources
- Sonnery-Cottet B, Carrozzo A, Poilvache H, et al. "Anterior cruciate ligament reconstruction combined with anterolateral ligament reconstruction using hamstring autograft versus anterior cruciate ligament reconstruction using bone–patellar tendon–bone autograft: a randomised controlled trial with 5-year follow-up." Lancet Reg Health Eur. 2026;62:101561. DOI: 10.1016/j.lanepe.2025.101561
- Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. "Anatomy of the anterolateral ligament of the knee." J Anat. 2013;223(4):321–328. DOI: 10.1111/joa.12087
- Getgood AMJ, Bryant DM, Litchfield R, et al. "Lateral Extra-articular Tenodesis Reduces Failure of Hamstring Tendon Autograft Anterior Cruciate Ligament Reconstruction: 2-Year Outcomes From the STABILITY Study Randomized Clinical Trial." Am J Sports Med. 2020;48(2):285–297. DOI: 10.1177/0363546519896333
- Saithna A, Daggett M, Helito CP, et al. "Clinical Results of Combined ACL and Anterolateral Ligament Reconstruction: A Narrative Review from the SANTI Study Group." J Knee Surg. 2021;34(9):962–970. DOI: 10.1055/s-0040-1701220
- AAOS OrthoInfo — Anterior Cruciate Ligament (ACL) Injuries