Computer-Guided Shoulder Replacement
Computer-guided total shoulder replacement — both anatomic and reverse — using 3D pre-operative CT planning and patient-specific instrumentation. The result is implant alignment placed from your actual scan, not estimated in real-time.
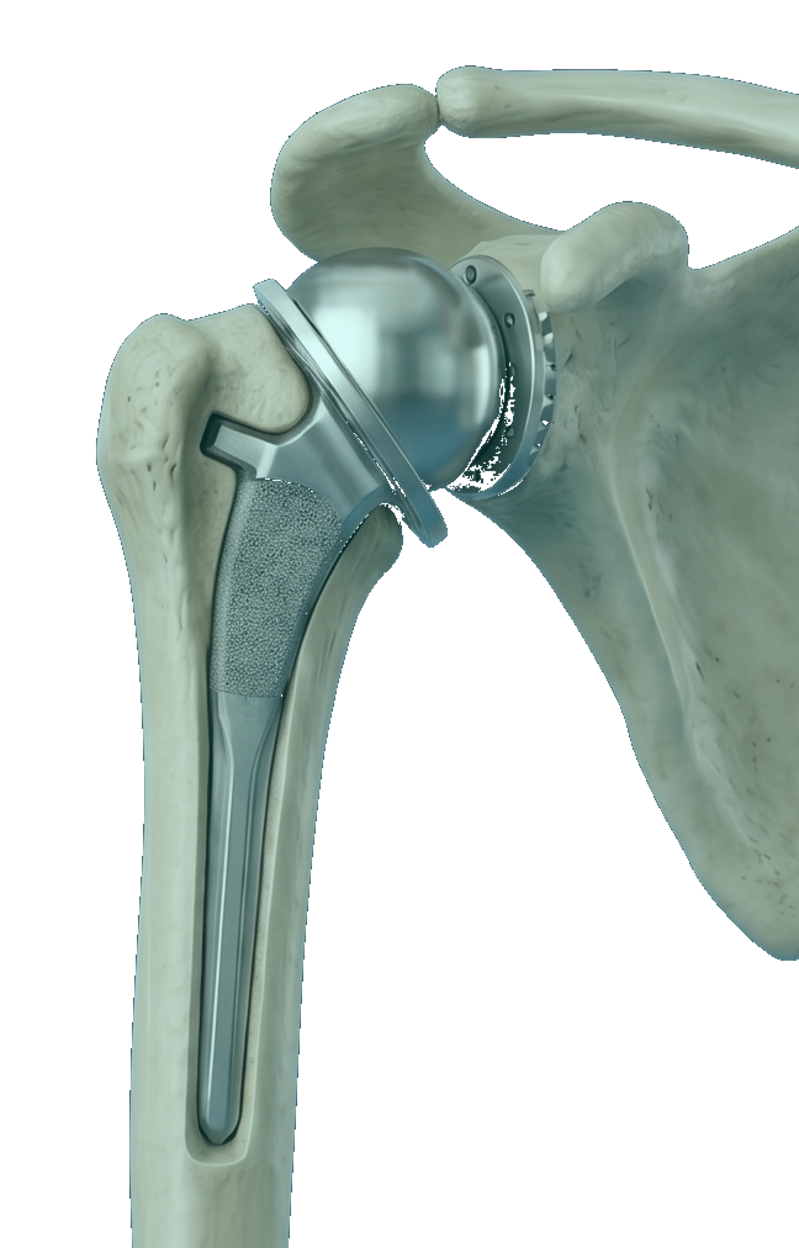
Shoulder replacement resurfaces the worn ball-and-socket joint between the humeral head (the ball at the top of the upper arm bone) and the glenoid (the socket on the shoulder blade). It is one of the most reliable surgeries in orthopedics for relieving the deep, mechanical pain of shoulder arthritis.
Anatomic shoulder replacement reproduces the natural anatomy: a metal ball replaces the humeral head, and a polyethylene socket replaces the glenoid. It is appropriate when the rotator-cuff tendons that drive shoulder motion are still intact.
Reverse shoulder arthroplasty inverts the anatomy — a metal ball is fixed to the scapula and a socket to the upper arm — so the deltoid muscle can power the shoulder when the rotator cuff is no longer functional. This is the procedure of choice for cuff-tear arthropathy and certain complex fracture patterns.
Patient-specific instrumentation from your own CT scan
Glenoid component placement is the technical heart of shoulder arthroplasty. A few degrees of malposition can change implant longevity. Dr. Dewan uses a CT-based 3D planning system to determine the exact glenoid version, inclination, and starting point that will best fit your anatomy.
Patient-specific instruments are then built from that plan. In the operating room, those instruments lock onto your scapula in only one orientation — the planned one — eliminating much of the guesswork that otherwise depends on intra-operative visual estimation.
The same CT data informs humeral component sizing and version, with the goal of restoring the natural ball-and-socket relationship rather than just substituting for it.
Computer-Guided Shoulder Replacement is most often considered for the following — though every situation is individualized.
- ▸Severe shoulder osteoarthritis with night pain or motion loss
- ▸Rotator-cuff arthropathy (reverse arthroplasty)
- ▸Avascular necrosis of the humeral head
- ▸Failed massive rotator cuff repair with secondary arthritis (reverse)
- ▸Complex three- or four-part proximal humerus fractures (reverse)
- ▸Inflammatory arthritis affecting the glenohumeral joint
A typical timeline.
Recovery varies by patient — these milestones are typical for an uncomplicated case. Dr. Dewan personalizes the plan to your starting point, goals, and surgical specifics.
- Day of surgerySling placed; interscalene block manages first-day pain
- Weeks 1–2Pendulum exercises start; sling worn outside the home
- Weeks 2–6Passive range-of-motion physical therapy; sling at night
- Weeks 6–12Active assisted and active range of motion; sling discontinued
- 3 monthsStrengthening begins; light overhead activity tolerated
- 4–6 monthsReturn to most recreational activities including golf and doubles tennis
What patients ask most.
How is reverse shoulder arthroplasty different from anatomic?+
In an anatomic shoulder replacement, the ball stays on the humerus and the socket stays on the scapula — recreating natural anatomy. In a reverse, the ball and socket are swapped: a ball is mounted on the scapula and a socket on the humerus. That mechanical change lets the deltoid drive shoulder elevation when the rotator cuff cannot. The choice depends entirely on the condition of your rotator cuff.
Read the full article→Why does computer-guided planning matter?+
Glenoid component position is the single biggest predictor of shoulder replacement longevity. CT-based planning lets Dr. Dewan see precisely where the glenoid is worn and plan version, inclination, and starting point accordingly — then patient-specific instruments execute that plan in the operating room with high reproducibility.
How long is the sling worn?+
Typically 4–6 weeks during the day, longer at night, depending on the procedure and your tissue quality. The sling protects the surgical repair while early healing happens. Pendulum exercises start almost immediately to prevent stiffness.
Will I be able to reach overhead again?+
Most patients regain functional overhead motion — meaning they can comfortably reach a high cabinet, brush hair, or do a tennis serve at recreational intensity. Final motion depends on your pre-operative range, the procedure performed, and your engagement with physical therapy.
Is shoulder replacement painful?+
An interscalene nerve block typically controls pain for the first 18–24 hours. After the block wears off, oral medications and ice are usually sufficient. Most patients report that the deep, mechanical, sleep-disrupting pain of arthritis is gone within days of surgery — long before the soft-tissue surgical soreness fully resolves.
Insights from sports medicine and orthopedic surgery.
Long-form patient education on the conditions and decisions related to computer-guided shoulder replacement.
Other operations Dr. Dewan does often.
Have a specific question about your case?
Every patient’s situation is different. The fastest way to know whether computer-guided shoulder replacementis right for you is a consultation — bring your imaging and a list of what you’ve already tried.