Arthroscopic Shoulder Reconstruction
Arthroscopic repair of the rotator cuff, labrum, and biceps tendon — the soft-tissue stabilizers and movers of the shoulder. The work happens through portal incisions, with suture anchors placed in bone and high-strength sutures restoring the torn tissue to its natural footprint.
Shoulder arthroscopy uses a small camera and miniature instruments inserted through portal incisions to address pathology inside the shoulder joint and the subacromial space above it.
The two most common reconstructions are: rotator cuff repair, where torn tendons are sutured back to the humeral head with bone-anchored sutures; and labral repair, where the fibrocartilage rim around the glenoid is reattached after a tear (Bankart for instability, SLAP for the superior labrum).
Other procedures include biceps tenodesis (relocating an inflamed long-head biceps tendon), subacromial decompression, distal clavicle excision for AC-joint arthritis, capsular shift or remplissage for recurrent shoulder instability, and the Latarjet procedure — transferring the coracoid bone block to the anterior glenoid — for complex instability with glenoid bone loss.
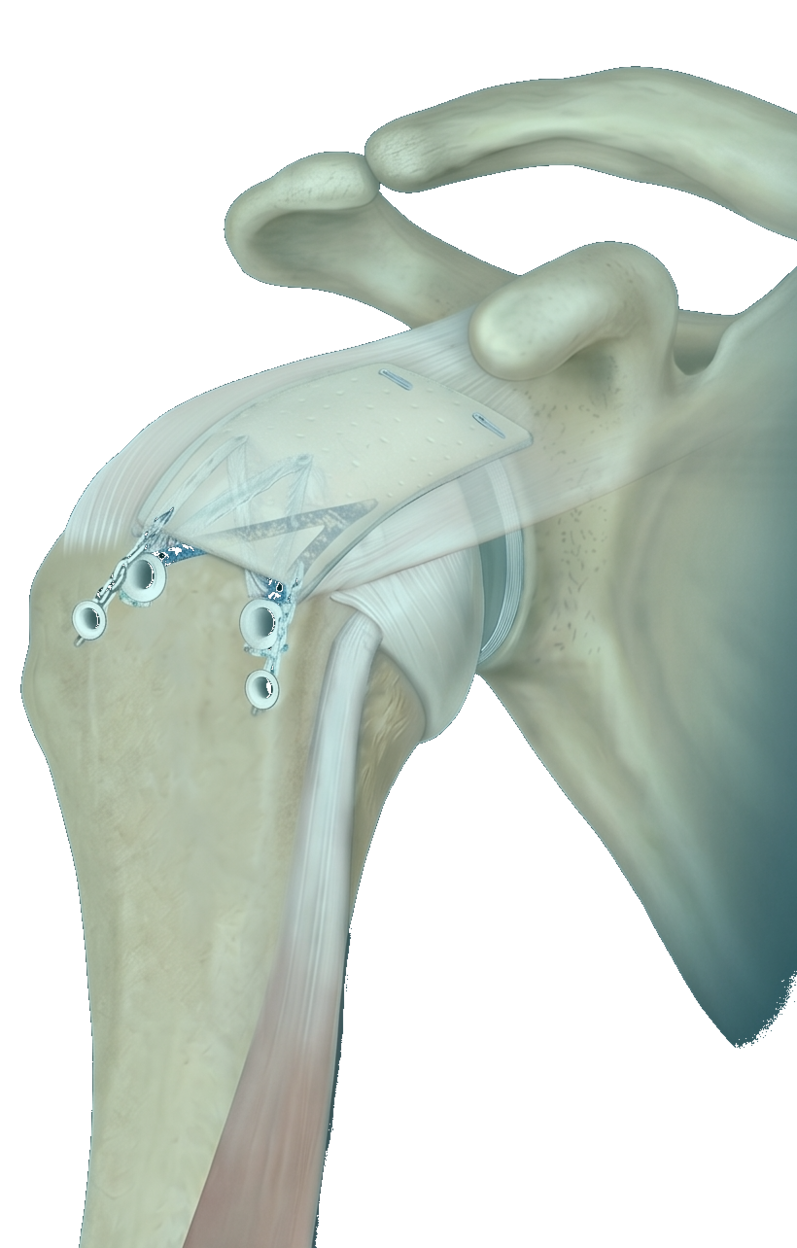
Anatomic footprint repair, durable fixation
For rotator cuff repair, Dr. Dewan uses a double-row construct when tear size and tissue quality allow — recreating the natural tendon footprint on the humerus. Bone-anchored sutures are passed through the tendon and tensioned to compress the tendon against bone for biological healing.
Labral repair restores the glenoid bumper that keeps the humeral head centered. For a Bankart lesion (anterior labral detachment from a dislocation), suture anchors recreate the labral attachment along the anterior glenoid. For a SLAP lesion (superior labrum biceps anchor), repair vs. tenodesis is decided based on age, sport demands, and tear pattern.
Throughout, the rotator cuff and capsule are preserved as much as possible — the goal is repair without unnecessary release of healthy structures.
Arthroscopic Shoulder Reconstruction is most often considered for the following — though every situation is individualized.
- ▸Rotator cuff tear (partial or full thickness, traumatic or degenerative)
- ▸Anterior labral tear / Bankart lesion after dislocation
- ▸SLAP tear (superior labrum, anterior to posterior)
- ▸Posterior labral tear (instability in football linemen, weightlifters)
- ▸Long-head biceps tendinopathy or tear
- ▸Subacromial impingement and bursitis
- ▸AC-joint arthritis with persistent symptoms
- ▸Recurrent shoulder instability
- ▸Complex instability with glenoid bone loss (Latarjet candidate)
A typical timeline.
Recovery varies by patient — these milestones are typical for an uncomplicated case. Dr. Dewan personalizes the plan to your starting point, goals, and surgical specifics.
- Day of surgerySling placed; interscalene block manages first-day pain
- Weeks 1–6Sling worn outside the home; pendulum exercises only
- Weeks 6–12Passive then active-assisted range of motion in physical therapy
- 3 monthsActive range-of-motion progression; sling discontinued
- 4 monthsStrengthening begins — rotator cuff and scapular stabilizers
- 6 monthsReturn to most overhead activities and contact sport (case-by-case)
What patients ask most.
Why is the rotator cuff repaired arthroscopically rather than open?+
Arthroscopic repair preserves the deltoid attachment to the acromion — a structure that an open approach has to detach and repair. Preserving the deltoid origin reduces post-operative weakness and shortens recovery. The biomechanics of the repair itself are equivalent or better arthroscopically when the surgeon is comfortable with the technique.
How long does a rotator cuff repair take to heal?+
Tendon-to-bone biology takes about 12 weeks for the initial repair to be biologically healed, and another 3–6 months for the construct to mature and remodel. That's why activity restrictions are progressive rather than single-step — early protected motion, gradual strengthening, and sport-specific return only after the tissue can take it.
Will I need a labral repair if I've dislocated my shoulder?+
First-time dislocations under age 25 with a traumatic mechanism have very high re-dislocation rates without surgery. Recurrent dislocations almost always warrant labral repair. Older patients with a single dislocation can sometimes manage non-operatively with rehab — Dr. Dewan reviews your imaging and risk profile to recommend a path.
What's the difference between SLAP repair and biceps tenodesis?+
A SLAP tear involves the superior labrum where the long-head biceps attaches. Younger overhead athletes with isolated labral pathology may do well with SLAP repair (suturing the labrum back). Patients over ~40, or with significant biceps tendinopathy, often do better with biceps tenodesis — relocating the biceps tendon out of the joint — because it eliminates the pain generator and avoids the post-op stiffness sometimes seen with SLAP repair.
Can I sleep on my side after surgery?+
Most patients sleep semi-reclined in a recliner or wedge for the first 2–4 weeks. Side-sleeping on the operative side is typically off-limits for 6 weeks. Many patients find sleep is the most uncomfortable part of early recovery — ice, position, and short-term sleep aids help.
Insights from sports medicine and orthopedic surgery.
Long-form patient education on the conditions and decisions related to arthroscopic shoulder reconstruction.
Rotator Cuff
3 articlesShoulder Labrum & Instability
3 articlesOther operations Dr. Dewan does often.
Have a specific question about your case?
Every patient’s situation is different. The fastest way to know whether arthroscopic shoulder reconstructionis right for you is a consultation — bring your imaging and a list of what you’ve already tried.