A paper in the New England Journal of Medicine made waves in orthopedic circles, and it's worth a careful read if you've been considering knee arthroscopy for a torn meniscus. The headline is striking: at 10 years of follow-up, the FIDELITY trial — a Finnish randomized study that compared arthroscopic partial meniscectomy (APM) against a placebo (“sham”) surgery for degenerative meniscus tears — found “no benefit and possible harm” from doing the operation.1
This matters because knee arthroscopy is one of the most commonly performed orthopedic operations in the United States — several hundred thousand per year — and a large share of those operations are for degenerative meniscus tears in adults in their 40s, 50s, and 60s. The 10-year FIDELITY data is the longest, highest-quality evidence we have on what those operations actually accomplish for the specific patient FIDELITY studied. The answer is increasingly clear, and it's not what a lot of people assume.
I want to walk you through what this study really shows, where it should change practice, and — just as important — what it does not show, because the nuance gets lost in headline summaries that read like “arthroscopy doesn't work.” That's a wrong oversimplification. Arthroscopy still does some of the most rewarding work in our field. It just doesn't do well at the specific job FIDELITY put it up against.
What the FIDELITY trial actually tested
If you remember nothing else from this article, remember this distinction: there are two very different kinds of meniscus tears, and the FIDELITY trial only studied one of them.
Degenerative tears
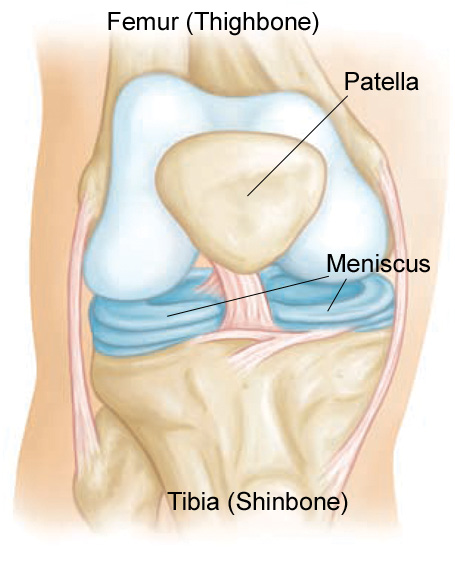
A degenerative meniscus tear is essentially the fraying that develops in the meniscus over years of normal use. It is part of the early spectrum of knee osteoarthritis. You typically cannot pin a date on it — there was no twisting injury, no pop, no instant swelling. The pain came on gradually, often with stiffness in the morning or aching after a long day on your feet. On MRI the meniscus looks ragged or frayed, most often in the back portion (the posterior horn) of the medial meniscus.
Acute traumatic tears
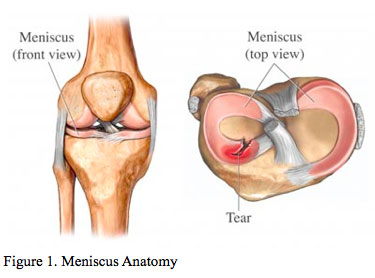
An acute traumatic tear is a sudden injury — usually a twist or a pivot — that causes immediate pain, swelling, and often a sense of something catching or locking inside the knee. These tears tend to have a cleaner pattern on MRI (a vertical, radial, or bucket-handle pattern) and they happen in younger, more active patients.
These two scenarios are not the same problem and they do not respond to the same treatment. The FIDELITY trial enrolled patients with degenerative tears — adults 35–65 years old, gradual onset, no acute injury, no mechanical locking, no advanced arthritis on X-ray. The trial design was the gold standard for surgical research: 146 patients were randomized to either real arthroscopic partial meniscectomy or to a sham procedure (the surgeon made the same skin incisions and inserted the scope, but did not remove any tissue). Patients and follow-up clinicians were blinded to which they had received. That is rare in surgical research — and it is exactly what you want when the question is “does the operation actually help, or are we mostly seeing the placebo effect of being operated on?”
The trial reported in stages. The original 12-month results were published in NEJM in 2013: no clinically meaningful difference between APM and sham.2 The 5-year follow-up appeared in Annals of Internal Medicine in 2018: still no difference, with a non-significant trend toward more radiographic arthritis progression in the surgical group.3 The 10-year follow-up — published in NEJM in April 2026 — is the longest sham-controlled follow-up we have for any orthopedic operation, and its conclusion is sharper.
The 10-year findings
At 10 years, the FIDELITY investigators report that participant-reported and radiographic outcomes “suggested no benefit and possible harm” from arthroscopic partial meniscectomy in this population. Three things matter:
Patient-reported outcomes showed no advantage to surgery
The standardized scores for knee pain, function, and disease-specific quality of life were essentially indistinguishable between the APM and sham groups. After a decade of follow-up the two groups look the same on every patient-reported axis. This is consistent with the 1-year and 5-year results — but with another decade of room for the surgical group to pull ahead, and they didn't.
Radiographic outcomes suggest the surgical group may have done slightly worse
Earlier follow-ups had shown a small, non-significant trend toward more cartilage loss and joint-space narrowing in the APM group. The 10-year data appears to strengthen that signal. Mechanically this fits a long-standing prediction: removing meniscus tissue increases the load funneled through the underlying cartilage, which over time accelerates the progression toward osteoarthritis. The FIDELITY 10-year data is the first sham-controlled evidence to suggest that prediction is playing out at a population level.
This caps a 15-year body of evidence pointing the same direction
The Moseley trial (NEJM 2002) had already shown arthroscopic debridement for knee osteoarthritis didn't outperform placebo. Multiple meta-analyses since 2014 have shown APM for degenerative tears doesn't outperform conservative care or sham. Major orthopedic societies (AAOS, ESSKA, the BMJ Rapid Recommendations group) have already issued recommendations against APM as first-line treatment for degenerative tears. The FIDELITY 10-year data is, frankly, what most of us in the field expected — but it's important confirmation.
What this study does well
Three things give the FIDELITY trial unusually high credibility, and they're worth understanding before you decide how heavily to weight its conclusions.
Sham control
Most “does this operation work?” studies compare a surgery against doing nothing, or against physical therapy. Both of those comparisons are confounded by the placebo effect of being operated on — the psychological “something is being done about my problem” effect is large for surgery and has been measured at 30% or more in some procedures. A sham control isolates the effect of the procedure itself from the broader effect of being a patient who had a surgical experience. Very few surgical trials in any field manage to pull this off, because patients and ethics boards reasonably object to “fake” surgery. That FIDELITY succeeded — and that the result has held up at 1, 5, and now 10 years — is a major scientific achievement.
Long follow-up
Most orthopedic randomized trials follow patients for six months or one year. Arthritis progresses over decades, so short follow-ups can miss the most important downstream consequences of a procedure — the question of whether removing meniscus tissue accelerates osteoarthritis cannot be answered in 12 months. Ten years is rare in our field. It gives the cartilage-acceleration concern enough runway to actually become visible.
Real-world relevance
The study population — adults 35–65 with knee pain and a degenerative tear on MRI but without acute injury or mechanical locking — is the exact patient who walks into clinic asking about arthroscopy. This is the patient FIDELITY answers for, and the recommendation matches the clinic-level question.

Important caveats — what the study does NOT prove
This is where the patient-education conversation gets nuanced. The FIDELITY trial is excellent, but a careful read clarifies exactly who its conclusion does and does not apply to. Several caveats matter.
It does not apply to acute traumatic tears
Patients explicitly excluded from FIDELITY: anyone whose tear was caused by a specific twisting injury, anyone with mechanical locking, anyone under 35. So if you're a 22-year-old soccer player who felt a pop when you cut at midfield and now your knee is locking — this study has nothing to say about you. Arthroscopic meniscus repair (sewing the torn fragment back into place — not removing it) is still strongly indicated in that scenario, and the long-term outcomes are excellent. See our walkthrough of a real arthroscopic bucket-handle meniscus repair for what that looks like in practice.
It does not apply to true mechanical symptoms
If your knee physically locks or catches because a flap of meniscus is getting trapped in the joint, FIDELITY excluded you and the result does not apply. Clicking or popping sounds without true locking is not the same thing — that's not what we mean by mechanical symptoms. But a knee that physically stops at, say, 90° and won't fully straighten is a different problem, and arthroscopy in that situation can be transformative.
It does not apply to repairable tear patterns
The trial studied partial meniscectomy — removal of the torn portion. Modern arthroscopy includes a fundamentally different operation, meniscus repair, where the torn fragment is sewn back into place using all-inside suture devices. Repair preserves the meniscus rather than removing it, and the long-term cartilage data is fundamentally different. FIDELITY did not test repair.
Sample size and crossover
146 patients is modest for detecting small effects. Some sham-arm patients eventually crossed over to APM, which dilutes the comparison. These don't undermine the main conclusion (the result is consistent with multiple other studies), but they're honest limitations worth knowing about.
“Possible harm” should not be over-read
Radiographic OA progression doesn't always translate to symptomatic OA. The 10-year paper signals harm at the imaging level. Whether that translates to more knee pain, earlier knee replacements, or worse quality of life at 15 or 20 years is still an open question that will need even longer follow-up. The word “possible” in the authors' conclusion is doing work.
What I tell my patients
So how does a working orthopedic surgeon actually use this evidence in clinic? When a patient comes in with knee pain and an MRI showing a meniscus tear, I walk through a sequence of questions.
1. Is the tear actually the source of the pain?
This is the most under-appreciated point. A torn meniscus on MRI does not automatically explain knee pain. Imaging studies have repeatedly found degenerative meniscus tears on MRI in 30–60% of asymptomatic middle-aged adults. The tear and the pain may be unrelated. A careful exam — sometimes supplemented by diagnostic injections — helps clarify whether the meniscus is the pain generator or an incidental finding.
2. Did the symptoms come on after a specific event?
If yes — an acute twist, a sudden pop, immediate swelling — your situation may be more like an acute tear than a degenerative one, and FIDELITY's conclusion may not apply directly. If no — a gradual onset of aching pain with morning stiffness — you fit the FIDELITY population.
3. Are there true mechanical symptoms?
True locking — the knee physically can't be straightened or bent past a certain angle — is a different problem and often does need arthroscopy. Clicking, popping, or a sense that the knee “gives way” without true locking is not the same and is less of a surgical indication.
4. Have you tried 8–12 weeks of structured non-operative care?
For the patient FIDELITY actually studied — middle-aged, gradual onset, no mechanical locking, no acute trauma — the right starting point is non-operative care for a meniscus tear: structured physical therapy, weight management (a 10-pound weight loss matters more than most patients realize — see the 5 strategies for joint pain piece for why), NSAIDs if you can tolerate them, activity modification, sometimes a corticosteroid or viscosupplementation injection. If you give that a fair trial and still aren't progressing, the conversation about arthroscopy is informed, but should still be cautious.
5. What do the weight-bearing X-rays show?
If your standing X-rays already show advanced osteoarthritis — bone-on-bone, significant joint space narrowing — the meniscus tear is a downstream finding and the arthritis is the real problem. Arthroscopy in advanced knee OA has been consistently shown not to help and may worsen progression. The right conversation in that situation is about whether knee replacement (now usually robotic-arm assisted — see robotic knee replacement) is the right next step. Arthroscopy is a detour.
The bottom line
Knee arthroscopy does some of the most rewarding work in our field — restoring stability after an acute ACL tear, repairing a bucket-handle meniscus that's locking up a young athlete, addressing impingement, accessing cartilage for restoration. None of that has changed with the FIDELITY 10-year data. What has changed — gradually, then with the new 10-year data, decisively — is the population for whom “I have a meniscus tear on MRI and I'm in my 50s” should be treated as an automatic indication for arthroscopy. The evidence is now overwhelming that for that specific patient, it isn't.
If you've been recommended an arthroscopy for what sounds like a degenerative tear without having tried structured non-operative care first, ask questions. A good surgeon will explain why the answer might not be surgery as readily as why it might be. If you'd like an independent read on your imaging and your situation, you can request a visit or call the office at (281) 690-4678.
Sources
- Kalske R, Sihvonen R, Paavola M, Malmivaara A; FIDELITY Investigators. “Arthroscopic Partial Meniscectomy for Degenerative Tear — 10-Year Outcomes.” N Engl J Med. 2026;394(17):1757–1759. DOI: 10.1056/NEJMc2516079
- Sihvonen R, Paavola M, Malmivaara A, et al. “Arthroscopic Partial Meniscectomy versus Sham Surgery for a Degenerative Meniscal Tear.” N Engl J Med. 2013;369(26):2515–2524. (Original 12-month FIDELITY results)
- Sihvonen R, et al. “Arthroscopic Partial Meniscectomy for a Degenerative Meniscus Tear: 5-Year Follow-up of a Randomized Trial.” Ann Intern Med. 2018;169(10):658–666.
- Moseley JB, et al. “A Controlled Trial of Arthroscopic Surgery for Osteoarthritis of the Knee.” N Engl J Med. 2002;347(2):81–88.
- Siemieniuk RAC, et al. “Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline.” BMJ. 2017;357:j1982. (BMJ Rapid Recommendations)
- AAOS OrthoInfo — Meniscus Tears