The anterior cruciate ligament (ACL) sits inside the knee joint with a limited blood supply. After it tears, it does not heal itself. The torn fragments may scar back together, but without the appropriate tension, the ACL is unable to provide anterior and rotatory stability to the knee. Historically attempts were made to repair the torn fibers directly with sutures, but this did not produce enough tension and ultimately failed. Newer research has focused on biological scaffolds and stem cells injected directly on the ACL to promote healing — but none of these approaches have made it to final clinical use. To restore knee stability, the current standard of care involves replacing your torn ligament with a substitute made of tendon. Tendon and ligaments are both made of collagen protein. When used for ACL reconstruction, the tendon is called the ACL graft. The graft serves as a scaffold on which new ligament tissue can grow.
Where the graft tissue comes from
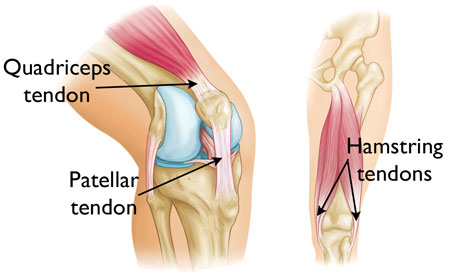
Tissue to reconstruct the ACL can be obtained from the same knee at the time of surgery, and in some cases from the opposite knee. The four commonly used sources are:
- Patellar tendon autograft (autograft = from the patient)
- Hamstring tendon autograft
- Quadriceps tendon autograft
- Allograft (cadaver tissue) — patellar, Achilles, semitendinosus, gracilis, or posterior tibialis tendon
Each graft type carries its own advantages and disadvantages. Choosing the right graft is part of the conversation we have when planning your surgery. The breakdown below covers the four most common options.
The four ACL graft options

Patellar tendon autograft (BPTB)
Gold standardOften referred to as the "gold standard" for ACL reconstruction. The middle third of the patellar tendon along with a piece of bone from the kneecap and shin bone is harvested from the front of the knee. Recommended for high-demand athletes and patients whose jobs do not require a significant amount of kneeling.
- Lowest graft failure rate (1.9%)
- Secure bone-block fixation in bone tunnels
- Anterior knee pain (17.4%), especially with kneeling
- Greater postoperative stiffness (6.3%)
- Rare risk of kneecap fracture

Hamstring tendon autograft
The hamstrings that can be used for ACL reconstruction attach to the inside aspect of the knee. Two tendons (the gracilis and semitendinosus) are harvested from the hamstring muscles and folded into a two- or four-strand graft.
- Less anterior knee pain (11.5%)
- Less postoperative stiffness (3.3%)
- Smaller incisions
- Faster early recovery
- Graft elongation (stretching) may occur
- Decreased hamstring strength
- Higher graft failure rate (4.9%)

Quadriceps tendon autograft
Revision-friendlyOften used as an alternative source of tissue when patients have failed a previous ACL reconstruction with another autograft. The middle third of the quadriceps tendon and a bone plug from the upper end of the kneecap are used.
- Secure bone-block fixation on one end
- Smaller incisions
- Anterior knee pain
- Rare risk of kneecap fracture

Allograft (cadaver tissue)
Cadaver grafts eliminate the need to harvest your own tissue. Until recently this was the go-to source for many surgeons, but newer studies have shown higher failure rates. Allograft tissue remains important for revision ACL reconstructions and multi-ligament repairs. Available types include patellar, Achilles, hamstring, and posterior tibialis tendons.
- No pain from graft harvest
- Shorter surgery time
- Smaller incisions
- Rare risk of disease transmission (HIV, Hepatitis C)
- Significantly higher failure rate (up to 23%) in young athletes
So which graft is right for you?
There is no universal "best" graft — the right choice depends on your age, activity level, occupation, prior surgical history, and what your knee anatomy will support. For a competitive cutting-and-pivoting athlete with no kneeling demands, BPTB autograft often wins. For a patient who kneels at work (electrician, flooring installer, religious observance), hamstring or quadriceps autograft may be a better fit. For revision cases or multi-ligament reconstructions, allograft can have a role. We talk through this together at your visit.
To see how the graft is actually implanted and secured, read on at ACL Reconstruction: A Patient's Guide.
Sources
- PubMed 15572332 — graft failure rates by autograft type
- PubMed 12531750 — BPTB vs hamstring outcomes
- PubMed 11912091 — anterior knee pain and kneeling after BPTB
- AAOS OrthoInfo — ACL injuries