Arthroscopic Knee Reconstruction
Arthroscopic surgery for ACL and other ligament reconstructions, meniscal repair, and cartilage restoration. The work is done through a few small incisions with a camera and miniature instruments — preserving the soft-tissue envelope around the joint so recovery is driven by the repaired structure, not the surgical access.
Knee arthroscopy uses a small camera (the arthroscope) inserted through portal incisions about the size of a pencil eraser. Through additional portals, miniature instruments repair, reconstruct, or restore the structures inside the joint. The damaged tissue is treated; the healthy tissue around it stays intact.
Common procedures include ACL reconstruction (where a torn ligament is replaced with a graft), Medial Patellofemoral Ligament (MPFL) reconstruction for patellar instability, meniscus repair or partial meniscectomy, articular cartilage restoration (microfracture, OATS, MACI), and treatment of loose bodies and other intra-articular pathology.
Repair where possible, reconstruct where necessary
For meniscus tears, Dr. Dewan repairs whenever the tear pattern, location, and tissue quality allow. Preserving the meniscus protects the articular cartilage long-term and is one of the most important predictors of avoiding future arthritis.
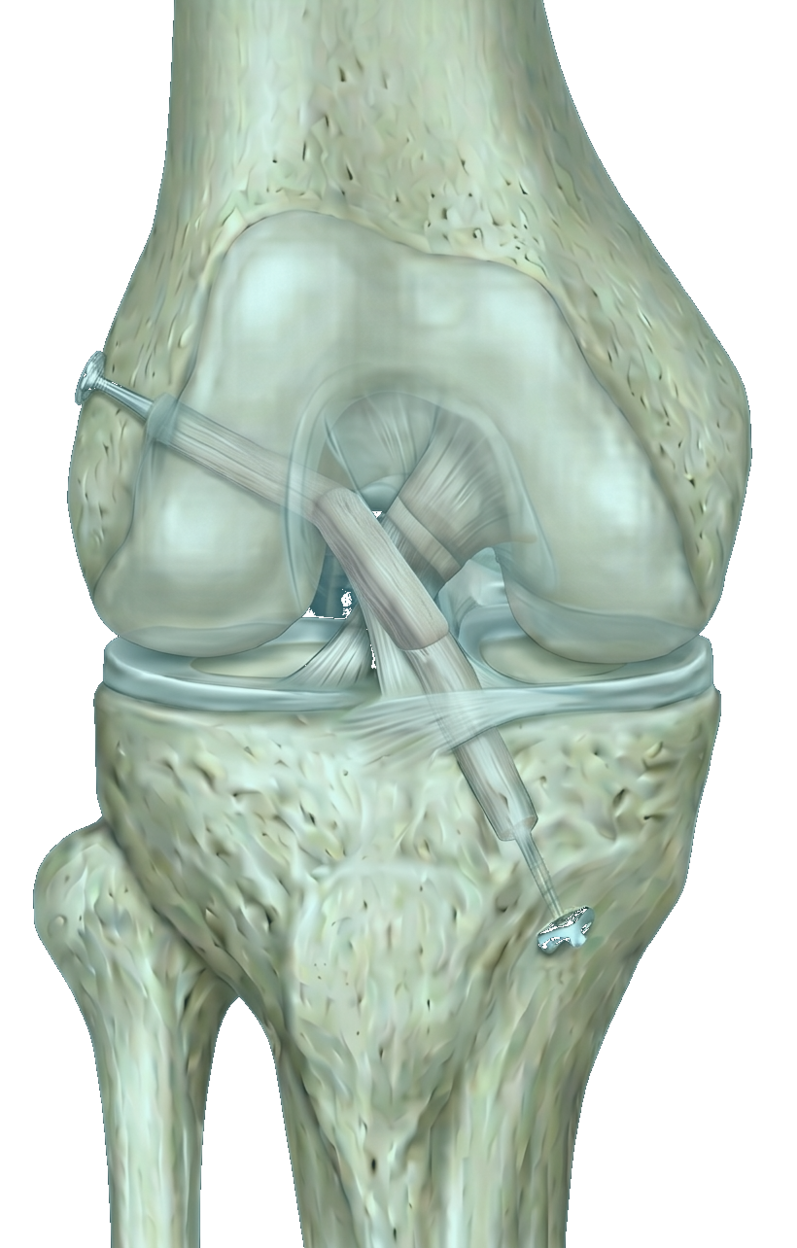
For ACL reconstruction, graft choice is individualized: hamstring autograft, patellar tendon (BTB) autograft, quadriceps tendon, or allograft, depending on your sport, age, and anatomy. Fixation uses cortical buttons (Tightrope) or interference screws — chosen for the bone tunnels and graft type.
For cartilage injuries, the technique is matched to the lesion: microfracture for small contained defects, osteochondral autograft (OATS) for medium full-thickness lesions, and matrix-induced autologous chondrocyte implantation (MACI) for larger defects. The goal is durable, hyaline-like cartilage rather than scar tissue.
Arthroscopic Knee Reconstruction is most often considered for the following — though every situation is individualized.
- ▸ACL tear (anterior cruciate ligament)
- ▸PCL, MCL, or LCL injury (often combined)
- ▸MPFL injury (medial patellofemoral ligament tear or recurrent patellar dislocation)
- ▸Meniscus tear — bucket-handle, root tear, complex tear
- ▸Articular cartilage defects from injury or osteochondritis dissecans
- ▸Patellar instability and dislocation
- ▸Loose bodies in the joint
- ▸Persistent mechanical symptoms (catching, locking) after non-operative treatment
A typical timeline.
Recovery varies by patient — these milestones are typical for an uncomplicated case. Dr. Dewan personalizes the plan to your starting point, goals, and surgical specifics.
- Day of surgeryOutpatient — home the same day with a brace and crutches
- Week 1Quad activation, ice, elevation; weight-bearing per your specific surgery
- Weeks 2–6Range-of-motion and gait normalization in physical therapy
- Weeks 6–12Strengthening — closed-chain, progressive load, hip and core
- 3–6 monthsSport-specific drills, agility, plyometric progression
- 9–12 monthsCleared return to cutting/pivoting sport for ACL reconstructions
What patients ask most.
What's the difference between ACL repair and ACL reconstruction?+
ACL repair is suturing the torn ends of the original ligament back together. It only works for very specific tear patterns (usually proximal avulsions in younger patients) and within a short window after injury. ACL reconstruction replaces the torn ligament with a graft — the more common and more durable option for most patients.
Which ACL graft should I choose?+
There's no single best graft for every patient. Hamstring grafts have minimal donor-site issues but slightly higher re-tear rates in young pivoting athletes. Patellar tendon grafts have excellent fixation strength and lower re-tear rates, with some risk of anterior knee pain. Quadriceps grafts are a middle ground. Allografts avoid donor-site morbidity but have higher re-tear rates in young athletes. Dr. Dewan reviews the trade-offs based on your sport, age, and prior injuries.
Will my meniscus tear be repaired or removed?+
Repair is preferred when the tear is in the vascular zone of the meniscus and the tissue is healthy enough to heal — preserving the meniscus is the single biggest factor in avoiding post-traumatic arthritis. Partial meniscectomy (removing only the torn portion) is reserved for tears that can't be repaired. Dr. Dewan makes this decision intra-operatively based on what the camera shows.
When can I return to sport?+
Meniscectomy: 4–6 weeks. Meniscus repair: 4–6 months. ACL reconstruction: 9–12 months for full cutting/pivoting clearance. Return-to-sport criteria are objective — strength symmetry, hop tests, agility — not just the calendar.
Will I need a brace?+
Bracing depends on the procedure. ACL reconstructions typically use a hinged brace for 4–6 weeks. Meniscus repairs in certain locations require a brace to limit deep flexion early. Simple meniscectomies and most cartilage procedures do not need a brace.
Insights from sports medicine and orthopedic surgery.
Long-form patient education on the conditions and decisions related to arthroscopic knee reconstruction.
ACL & Knee Ligaments
6 articlesMeniscus & Cartilage
3 articlesPatellar Instability
2 articlesOther operations Dr. Dewan does often.
Have a specific question about your case?
Every patient’s situation is different. The fastest way to know whether arthroscopic knee reconstructionis right for you is a consultation — bring your imaging and a list of what you’ve already tried.