A new kind of knee implant has been making the rounds in the lay press, in orthopedic society newsletters, and — most importantly for me — in clinic. Several patients in the past month have walked in with a printout of an article asking some version of the same question: “Is this thing the answer? Can I get this instead of a knee replacement?”
The device is called the MISHA Knee System (Moximed), and the news pegged to it is real: the FDA cleared it for medial-compartment knee osteoarthritis in 2023, the AAOS announced a category-1 CPT billing code that goes live January 1, 2027, the manufacturer recently released 5-year survivorship data, and a head-to-head randomized trial against non-surgical care began enrolling patients in May 2026.1,2
So it's not vaporware. But the gap between “FDA-cleared with promising single-arm data” and “ready to replace knee replacement” is wide, and that gap is where most of the patient conversations land. I want to lay out, plainly, what the device does, what the evidence actually shows, where the evidence is thin, who the legitimate candidate is, and how I'm thinking about it in clinic.
What the MISHA Knee System actually is
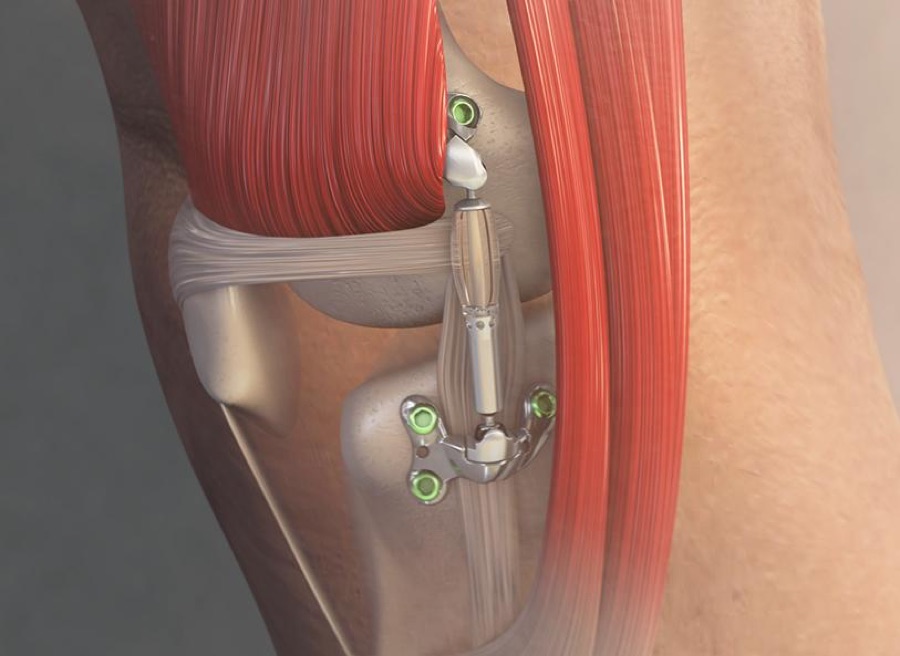
The MISHA is not a partial knee replacement. It does not enter the knee joint at all. It is a small mechanical shock absorber — a steel piston gliding inside a polymer cylinder — that gets attached to the outside of the leg with two titanium plates: one anchored to the inner side of the femur (thighbone), one to the inner side of the tibia (shinbone). It sits in the subcutaneous tissues just under the skin, parallel to the medial collateral ligament, and shortens and lengthens with every step the way the medial joint already does.3
The mechanical idea is straightforward. The medial side of the knee carries about 70% of the load when you stand on one leg, and in medial-compartment osteoarthritis the cartilage on that side is what wears down. Engineering studies of the device estimate it offloads roughly 30% of the peak medial compartment force per step — about 90 pounds for a 200-pound patient walking at normal speed.3 The body's own anatomy keeps doing the rest.

The procedure itself is a single small incision on the inner side of the knee, outpatient, no bone resection inside the joint, and recovery to full weight-bearing reported at a median of ~13 days in published series — compared to ~58 days for a high tibial osteotomy (which is the closest comparable joint-preserving surgery) and several months of structured rehab for a knee replacement.4
The implant is also marketed as reversible — meaning if it doesn't work, it can be removed, and the patient is theoretically still a candidate for a future osteotomy or arthroplasty. That's true in principle. We'll come back to whether it's quite as clean as it sounds.
What the published evidence actually shows
The evidence base that supports the FDA clearance and the marketing claims comes from a series of overlapping studies funded and conducted by Moximed or by surgeons with financial relationships to the company. The most-cited papers are:
- Gomoll et al., Knee Surgery, Sports Traumatology, Arthroscopy (2023) — a pooled analysis combining three Moximed-sponsored prospective single-arm studies. N = 171 patients with medial-compartment OA, working-age (mean age in the 50s), all treated with the implant. Primary outcome: survival from arthroplasty (i.e., not converting to a knee replacement) at 5 years. Reported result: 85%.5
- Pareek et al., Cartilage (2023) — a retrospective comparison in patients with high-risk Subchondral Insufficiency Fractures of the Knee (SIFK) showing 100% freedom from arthroplasty conversion at 2 years with the implant vs. 0% in a matched non-surgical group — but with very small numbers and the inherent selection bias of a retrospective design.6
- Raji et al., Video Journal of Sports Medicine (2025) — case report and indirect comparison reporting 95.8% pain relief in the MISHA group vs. 87.9% in a high tibial osteotomy group, and dramatically faster return to weight-bearing.4
- Manufacturer 5-year update (2026) — single-arm follow-up of 81 patients reporting 90.1% treatment survivorship, 95.7% clinically meaningful improvement in WOMAC pain scores, and 11/81 (13.6%) implant removals for discomfort, infection, or dissatisfaction.1
And, fresh from May 2026: the MOTION randomized controlled trial just enrolled its first patients. MOTION is a prospective, multicenter trial comparing the MISHA against the AAOS-guideline-based non-surgical package (weight loss, PT, injections, NSAIDs, braces). It is the first randomized comparison the device will face. It will run for years.2
What's genuinely strong here
I want to be fair to the evidence. There are real strengths.
- The biomechanical case is sound. Reducing medial compartment load by ~30% with every step is a meaningful intervention in a joint where the disease is fundamentally mechanical.
- The 5-year survivorship looks decent. If 85–90% of treated working-age patients are still implanted and out of an arthroplasty at 5 years, that's a clinically useful number.
- The recovery profile is fast. ~13 days to full weight-bearing in an outpatient procedure is genuinely attractive for active patients who can't take 3–6 months out of their lives.
- It does not burn any bridges anatomically. Because nothing is taken out of the knee, the patient remains a candidate for high tibial osteotomy, partial knee replacement, or total knee replacement if the device fails.
- An RCT is finally happening. The MOTION trial is the right next step. Even better, the comparator (AAOS-guideline non-op care) is the right thing to compare to for the patient population most likely to be offered the device.
Where the evidence is genuinely thin
This is where the article matters, because most coverage of the device skips this section. A careful patient or referring physician should not.
- Industry funding everywhere. The studies that underpin the FDA clearance and the marketing claims were either funded by Moximed or conducted by investigators with financial relationships to Moximed (stock options, consulting agreements, royalty arrangements). That doesn't automatically invalidate the data, but it does mean the evidence has been generated by people with a stake in the answer, and conclusions should be weighted accordingly.4
- No head-to-head randomized trial against knee replacement. The case in the lay press is “this might let you avoid or delay a knee replacement.” That is exactly the question that has not been answered. The MOTION RCT compares MISHA to non-surgical care, which is a different question. A MISHA-vs-TKA or MISHA-vs-UKA (partial knee replacement) trial does not exist.
- The 5-year data is single-arm. The 85–90% survivorship number sounds great until you ask: what would the same patients have done with non-op care alone, or with a partial knee replacement, or with a high tibial osteotomy? Without a comparator, we can't answer that.
- The reported populations are heavily selected. Medial-compartment-only OA, working age, motivated, intact ligaments, no significant deformity. That's perhaps 10–15% of the patients I see for “knee arthritis.” The other 85% — bone-on-bone tricompartmental disease, severe varus deformity, prior surgeries, complex coexisting pathology — are not candidates and never were in the studies.
- 13.6% explant rate is a real number. Out of the most recently published 5-year cohort, 11 of 81 patients had the device removed (discomfort, infection, dissatisfaction). 15 total complications were reported. That is not catastrophic, but it is also not nothing, and the patient signing up for “a quick outpatient procedure” should know that roughly 1 in 7 of them in the published series ended up having a second operation to take it out.
- Reversibility is a softer claim than it sounds. Yes, the device can be removed. But the holes drilled in the femur and tibia for the anchor plates are still there. They heal, but they alter the bone, and they can complicate a future arthroplasty's planning. Reversibility is not the same as “leaves no trace.”
- What happens to the other compartments? If we offload the medial side by 30%, mechanically that load has to go somewhere. Whether long-term unloading accelerates lateral compartment or patellofemoral wear remains an open question that 5-year data is too short to fully answer.
- The cost is non-trivial and the value case isn't settled. The implant and procedure are expensive, the AAOS-blessed CPT code goes live in 2027, and insurance coverage is patchwork. For most U.S. patients in 2026, this is partially or fully out-of-pocket. Whether the cost is justified by the benefit — relative to delaying surgery, or to going straight to a partial knee replacement that has decades of evidence — is unproven.
How I'm thinking about it in clinic
I take new technology seriously, and I do not dismiss a device just because the evidence is early. Partial knee replacement, robotic-arm-assisted total knee replacement, and arthroscopic meniscus repair all went through periods like this — promising biomechanical case, single-arm data, vocal early adopters, hesitant majority. Some of those technologies became standard. Others didn't.
My current read on the MISHA, said plainly:
It is reasonable to discuss for a specific kind of patient. That patient is a working-age adult (roughly late 40s through early 60s), with strictly medial-compartment osteoarthritis, intact ligaments, no significant fixed deformity, who has failed an adequate course of non-operative care (weight management if applicable, structured physical therapy, NSAIDs, an injection trial), who is otherwise too active to accept the recovery of a knee replacement, and who has been counseled in detail about what the evidence does and does not show. That patient is uncommon — but they exist, and for them the device is a defensible option to put on the table.
It is not a substitute for knee replacement in patients who actually need a knee replacement. If your imaging shows bone-on-bone disease across the joint, if your knee is significantly bowed in or out of alignment, if your ligaments are loose, if you've had prior interventions that have failed — the MISHA is not the answer. The answer for that patient is a partial or total knee replacement, and the question to focus on is which surgeon, which technique, and which timing.
It is reasonable to wait for the MOTION RCT. Patients who are on the fence about a procedure with single-arm 5-year data and no head-to-head comparison have a perfectly valid reason to keep the device in the “watching this space” column for another 2–3 years while better evidence accumulates. Non-operative care done well is durable. The window to revisit will still be open.
Bottom line for the layperson
- The MISHA Knee System is real and FDA-cleared. It's a small mechanical shock absorber implanted outside the knee joint to offload the medial side, for early- to mid-stage medial-compartment osteoarthritis only.
- The published evidence is promising but limited. ~85–90% of patients in single-arm 5-year studies have avoided knee replacement. About 1 in 7 had the device removed. None of that comes from a comparison against actually getting a knee replacement.
- The first randomized trial is just starting. The MOTION RCT will compare the device against non-surgical care. Results are years away.
- It is not a replacement for knee replacement. For most patients with significant arthritis, especially bone-on-bone or multi-compartment disease, the mature evidence base for partial or total knee replacement still wins.
- If you're considering it, get a careful evaluation. The right patient for this device is a narrow slice of the population with knee arthritis. The wrong candidate gets an expensive procedure that delays the correct one. Bring your imaging to a consult and have the full conversation — non-op options, partial knee replacement, total knee replacement, osteotomy, MISHA — laid out side by side.
References
- Healio Orthopedics. Implantable shock absorber may relieve pain, improve function in medial knee OA. May 21, 2026.
- Moximed press release. First Patients Treated in a New Randomized Controlled Trial Evaluating the MISHA Knee System vs Non-Surgical Treatment for Knee Osteoarthritis. May 2026. moximed.com
- Arthritis Foundation. FDA Clears New Implant for Knee OA. arthritis.org
- Raji Y, Topkarci B, Vel MS, Andersen W, Putko RM, Sherman SL. Medial Implantable Shock Absorber (MISHA) to Treat Medial Knee Arthritis in an Active Patient. Video Journal of Sports Medicine. 2025;5(3):26350254241303558. doi:10.1177/26350254241303558
- Gomoll AH, Diduch DR, Flanigan DC, Ranawat AS, Slynarski K, Walawski J, Crawford DC. Implantable shock absorber yields 85% survival from arthroplasty at 5 years in medial compartment knee osteoarthritis. Knee Surgery, Sports Traumatology, Arthroscopy. 2023. doi:10.1007/s00167-023-07373-4
- Pareek A, Parkes CW, Gomoll AH, Krych AJ. Implantable Shock Absorber Treatment in High-Risk SIFK Patients. CARTILAGE. 2023. doi:10.1177/19476035231154513
This article reflects Dr. Dewan's reading of the cited evidence at the time of publication. It is educational content, not medical advice. Your specific case may differ — schedule a consultation to discuss your imaging and history.