
When patients finally come in to talk about surgery for a torn rotator cuff, it is often the disrupted sleep that gets them in my office. They tell me they haven't had a full night's rest in months — that they can't lie on the bad side, that the ache wakes them at two in the morning, that they've migrated to the recliner and their spouse has stopped asking when they're coming back to bed. So the question they really want answered is simple and human: “If I do this, will I sleep through the night again?”
Here is the headline, and it is genuinely good news. Across multiple studies, disturbed sleep is one of the symptoms that responds most reliably to rotator cuff repair. In the largest recent series — 973 patients — the share with disturbed sleep fell from 88% before surgery to 37% at six months and 22% at one year.1 The catch, and the part most marketing copy skips, is the timeline: it often gets worse for the first several weeks before it gets reliably better.
Why a torn cuff wrecks your sleep in the first place
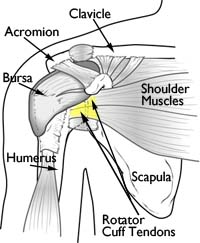
The rotator cuff is the group of four tendons that wrap the top of the arm bone and hold the ball of the shoulder centered in its socket. When one of those tendons is torn or badly inflamed, two things conspire against sleep. First, lying down removes the small amount of support that an upright posture and your arm-by-your-side give the joint, so the torn tendon and the inflamed bursa get tugged and pinched in positions that feel fine during the day. Second, there's a circulation rhythm to it — blood flow and the body's own anti-inflammatory signals dip overnight, which is part of why so many joint and tendon problems are at their loudest in the small hours. Roll onto the bad shoulder and the pain is immediate; even lying flat on your back can let the arm drift into a position that aches.
This is not a rare complaint. Roughly 70% of people with a significant shoulder disorder report meaningful trouble sleeping, and in surgical series the number is higher still — around 88–89% of patients heading into rotator cuff repair score in the disturbed-sleep range on standard questionnaires.12 If you feel like the tear has hijacked your nights, you are squarely in the majority.
What the studies actually did
The useful thing about this question is that several independent groups have measured it the same careful way: they enrolled patients before surgery, scored their sleep with a validated tool, and then re-scored the same patients at set points afterward — so each person serves as their own comparison.
The classic study is Austin and colleagues (2015), who followed 56 patients with full-thickness tears and scored sleep with the Pittsburgh Sleep Quality Index — a standard questionnaire — at 2, 6, 12, 18, and 24 weeks after repair.2 A much larger prospective, multi-center cohort by Feltri and colleagues (2025) tracked 973 patients out to a year.1 Zheng and colleagues (2023) followed 293 patients for a full two years to ask a different question: does sleep stay fixed, and do the patients who sleep better also recover better overall?3 Finally, a 2025 systematic review by Daher and colleagues pooled 13 studies and 2,447 patients to pin down when, on average, the improvement actually shows up.4
What they found
Sleep improves a lot — and the gains are durable
The direction is consistent across every study. Feltri's 973-patient cohort is the cleanest snapshot: 88% disturbed before surgery, 37% at six months, 22% at one year.1 Austin's smaller series found that only 38% of patients still had disturbed sleep at six months, down from 89%.2 And Zheng's two-year follow-up shows the fix tends to hold: 84% of patients who came in with disturbed sleep reported it resolved by two years.3

The turn comes around three months — not the first week
This is the number patients most need and least often hear. Daher's review of 2,447 patients found that a meaningful improvement in sleep is detectable by three months, and it keeps building at six and twelve months.4 Austin's data agree: the first statistically significant jump showed up at the three-month mark and continued through six months.2 What no study shows is overnight relief. The repaired tendon has to heal to the bone, the arm spends weeks in a sling, and the early post-operative period is its own source of pain.
Better sleep travels with better recovery
Zheng's group found that the patients whose sleep resolved also posted better shoulder-function scores than those whose sleep stayed disturbed.3 Sleep is not just a comfort metric — it tracks with how the whole shoulder is doing.
What these studies do well
Two features make this body of evidence trustworthy for a patient decision.
They followed the same patients over time
Because each person's after-surgery sleep is compared with their own before-surgery sleep, these studies sidestep a lot of the noise that plagues research comparing different groups of people. When someone goes from a disturbed score to a normal one, that change is hard to argue with.
Small studies and big ones point the same way
A 56-patient series from 2015, a 973-patient cohort from 2025, and a 2,447-patient pooled review all land on the same story: large improvement, mostly realized between three and twelve months. When independent studies of very different sizes agree, you can lean on the conclusion.
Where I'd push back on an over-simple reading
“Surgery fixes the sleep” is true on average, but a patient deserves the asterisks.
It gets worse before it gets better
None of these studies measured the first few nights, and that's exactly when patients are most shocked. The freshly repaired shoulder hurts, you're locked in a sling, and you cannot lie on that side or flat on your back without the arm settling into an unhappy position. Most people sleep upright in a recliner or propped on a wedge for the first few weeks. If you expect to sleep better the night you get home, you'll be discouraged. Picture a dip, then a climb.
The measuring sticks aren't identical
One study used the Pittsburgh index, another a single sleep question, another a yes/no on disturbance. Daher's reviewers flagged this head-on: the studies are statistically “noisy” because they measured sleep differently, and most are observational rather than randomized.4 The trend is robust; the exact percentages should be read as approximate.
Painkillers can sabotage the very sleep you're chasing
Austin's group found that prolonged opioid use after surgery was associated with worse sleep, not better.2 Narcotics fragment sleep architecture even when they dull pain. This is a real tension in the early weeks, and it shapes how I manage post-operative pain.
Not everyone recovers on the same clock
In Feltri's cohort, women reported worse sleep quality at follow-up than men, and a minority of patients in every study still had disturbed sleep at a year.1 Larger tears, stiffer shoulders, and other pain generators — a cranky neck, the opposite shoulder — can all slow the timeline. “Most patients” is not “all patients.”

What this means in my practice
When a patient asks me whether they'll sleep again, I give them the two-part answer the evidence supports — the reassurance and the realism.
1. Yes, and it's one of the most reliable wins of the operation
Of everything rotator cuff repair does, restoring sleep is among the things I'm most confident promising — not because I'm optimistic, but because the data are unusually consistent. The large majority of patients who come to me sleep-deprived are sleeping through the night within a few months. For many, this is the single change that makes them feel like themselves again.
2. Plan for a rough first month, on purpose
I tell patients before surgery to set up a recliner or a foam wedge at home, because they will likely sleep semi-upright with the sling on for the first several weeks. Knowing this in advance changes how people interpret it: a hard early stretch you were warned about reads as “on schedule,” not “something went wrong.” A pillow under the elbow takes the drag off the repair, and ice before bed helps. Lying flat on the back, and lying on the operated side, come later.
3. We manage pain to protect sleep, not just to numb it
Because prolonged narcotics are linked to worse sleep, I lean on a multi-modal plan — scheduled anti-inflammatories where they're safe, ice, nerve blocks at the time of surgery, and the shortest reasonable course of stronger medication — with the explicit goal of getting patients off opioids early. The point isn't to be stingy; it's that the medication that masks pain at 10 p.m. can be the same thing waking you at 3 a.m.
4. Who this timeline fits — and who it doesn't
The studies here are adults with degenerative or traumatic cuff tears going to arthroscopic repair, which is the bulk of my shoulder practice (see arthroscopic shoulder reconstruction). If your tear is very large or retracted, if your shoulder is already stiff, or if a good chunk of your night pain is actually coming from your neck or the other shoulder, your curve may be slower or partial — repairing one tendon can't fix a problem somewhere else. That's a conversation to have with your imaging in front of us.
5. When lost sleep after surgery deserves a second look
A dip in the first weeks is expected. What isn't: night pain that is escalating months out, or new fevers, spreading redness, or drainage — those are checked promptly, not slept through. Evidence suggests the overwhelming majority of post-repair sleep trouble is the normal healing curve. A good follow-up exists to catch the rare case that isn't.
The bottom line for the layperson
- Lost sleep is the most common reason people finally fix a torn rotator cuff — and it's one of the symptoms surgery improves most reliably.
- In the largest study, disturbed sleep fell from 88% of patients before surgery to 37% at six months and 22% at one year. The improvement tends to last.
- Expect it to get worse before it gets better. The turn usually comes around three months, not the first week.
- Plan to sleep propped up in a recliner or on a wedge with the sling on for the first several weeks. A pillow under the elbow and ice before bed help.
- Long courses of strong painkillers can worsen sleep — so good pain management aims to get you off them early, not just to numb the shoulder.
If night pain from your shoulder is what's wearing you down — or you're weighing rotator cuff surgery and the sleep question is the one holding you back — that's a reasonable conversation to have in person. You can request a visit or call the office at (281) 690-4678.
Sources
- Feltri P, Audigé L, Candrian C, Mueller AM, Fritz Y, Filardo G. “Rotator cuff repair: Sleep disturbance significantly improves after arthroscopic tendon repair.” Knee Surg Sports Traumatol Arthrosc. 2025;33(4):1459–1471. DOI: 10.1002/ksa.12420 (PMID: 39189149)
- Austin L, Pepe M, Tucker B, Ong A, Nugent R, Eck B, Tjoumakaris F. “Sleep disturbance associated with rotator cuff tear: correction with arthroscopic rotator cuff repair.” Am J Sports Med. 2015;43(6):1455–1459. DOI: 10.1177/0363546515572769 (PMID: 25776185)
- Zheng ET, Lowenstein NA, Collins JE, Matzkin EG. “Resolution of Sleep Disturbance and Improved Functional Outcomes After Rotator Cuff Repair.” Am J Sports Med. 2023;51(7):1852–1858. DOI: 10.1177/03635465231169254 (PMID: 37167606)
- Daher M, Parmar T, Boufadel P, Fares MY, Khan AZ, Horneff JG, Abboud JA. “Improvement of Sleep Disturbance After Rotator Cuff Repair Occurs at 3 Months.” Orthop J Sports Med. 2025;13(12):23259671251397512. DOI: 10.1177/23259671251397512 (PMID: 41426262)
- AAOS OrthoInfo — Rotator Cuff Tears
This article reflects Dr. Dewan's reading of the cited evidence at the time of publication. It is educational content, not medical advice. Your specific case may differ — schedule a consultation to discuss your imaging and history.