One area of controversy in shoulder surgery is when to perform a glenoid (shoulder socket) augmentation procedure for shoulder instability. Joint stability is dictated by the bony anatomy, the surrounding ligaments, and the supporting muscles. After a shoulder dislocation it’s common to tear the labrum (see Shoulder Labral Tears: Relevant Anatomy and Function). Sometimes the shoulder socket itself can also be damaged in the process, and the lip of the glenoid can break off.
When the glenoid surface area is reduced, the shoulder becomes more inherently unstable. When a large portion of bony socket is involved, repairing the rim is essential. When only a small portion is involved, it’s less clear-cut — and that’s where the surgeon community disagrees.
The two procedures most commonly debated are arthroscopic Bankart repair (labral repair alone, using suture anchors) and the open Bristow-Latarjet bone-block procedure (transferring a piece of the coracoid bone with its conjoined tendon to augment the front of the glenoid socket). Here’s how I think about them.
Arthroscopic Bankart vs open Latarjet
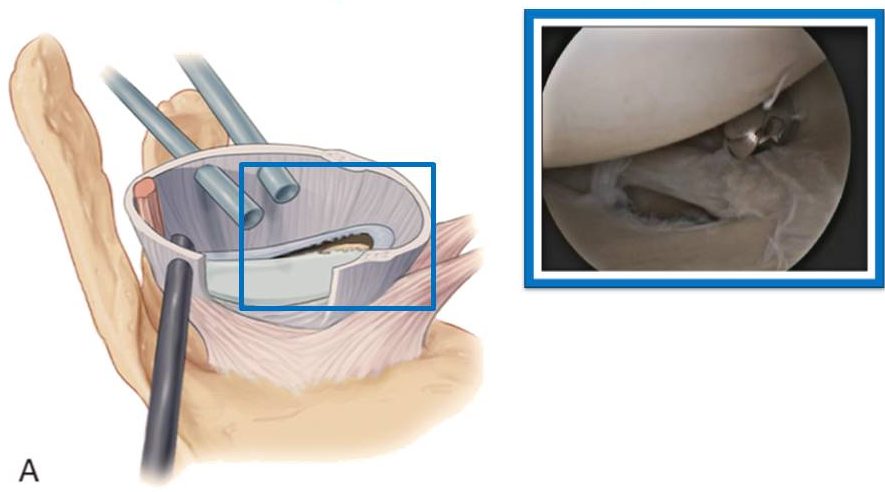
Arthroscopic Bankart repair
First-lineMinimally invasive arthroscopic procedure that re-attaches the torn anterior labrum to the glenoid rim using small suture anchors. Best suited for patients with intact glenoid bony anatomy and no significant bone loss.
- Minimally invasive — small portal incisions only
- Better return-to-sport rate (Blonna et al.)
- Better external rotation in the throwing position
- Better subjective shoulder perception
- Small trend toward higher re-dislocation rate when bone loss is present
- Not appropriate when glenoid bone loss exceeds ~20%
- Patients with hyperlaxity may still feel unstable
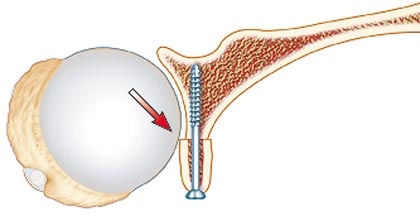
Bristow-Latarjet bone-block
Bone loss / revisionOpen procedure that transfers a piece of the coracoid bone (with its conjoined tendon attachment) to the anterior glenoid, restoring the lost bony surface area and providing a dynamic sling effect from the conjoined tendon.
- Addresses true bony deficiency, not just soft tissue
- Lower re-dislocation rate in high-bone-loss shoulders
- Dynamic sling effect from the conjoined tendon
- Procedure of choice for failed prior labral repair
- Open procedure, more morbid recovery
- Slower return to sport vs arthroscopic repair
- Reduced external rotation in throwing position
- Hardware (screws) in the joint long-term
How I decide
A recent matched-pairs study by Blonna et al. (American Journal of Sports Medicine, 2016) tackled the controversy head-on. The authors concluded that arthroscopic Bankart repair using anchors provided better return to sport, better external rotation in the throwing position, and better subjective perception of the affected shoulder compared to the open Bristow-Latarjet. There was a small (non-statistically-significant) trend toward higher re-dislocation rate with the arthroscopic repair — a difference that might have reached significance with a larger sample.
For athletes trying to get back on the field, fast and safe return-to-play is the most relevant concern. In my own practice, when the bone socket has minimal damage, my preference is still to perform the less morbid arthroscopic labral repair. If the shoulder re-dislocates after labral repair — or if the imaging shows significant glenoid bone loss up front — the bone-block procedure becomes more appealing.
This study’s conclusion supports that staged approach. More work needs to be done before we can arrive at a definitive consensus, but the framework is durable: soft-tissue first when soft-tissue is the problem; bone augmentation when bone is the problem.
Source
- Blonna D, et al. Arthroscopic Bankart Repair Versus Open Bristow-Latarjet for Shoulder Instability: A Matched-Pair Multicenter Study Focused on Return to Sport. Am J Sports Med 2016. Read the abstract.