If your shoulder is wearing out and a replacement is on the table, you will quickly run into a fork in the road: anatomic total shoulder replacement or reverse total shoulder replacement. They sound like variations on the same operation. They are not. They rebuild the joint in opposite ways, and the right answer depends mostly on one structure you cannot see in the mirror — your rotator cuff.
For most of the last twenty years the teaching was simple: a working rotator cuff means an anatomic replacement; a torn or worn-out cuff means a reverse. That rule still holds at the two ends. What has changed — and what is worth a careful read if you are facing this decision — is the large middle ground. National joint registries and a run of 2024–2025 analyses now show that the reverse design fails and needs revision less often than the anatomic one, even in shoulders with a perfectly good cuff.1 That has nudged a lot of surgeons toward reverse replacements in patients who, a decade ago, would have automatically gotten an anatomic one.
Here is what the two operations actually are, what the evidence does and does not say, and how I walk a patient through the choice in clinic.
Two operations, one swapped part
A healthy shoulder is a ball-and-socket joint: the ball is the top of your arm bone (the humeral head), and the socket is a shallow dish on the shoulder blade called the glenoid. Wrapped around that ball is the rotator cuff — four tendons that both hold the ball centered in its shallow socket and do much of the work of lifting and rotating your arm.
Anatomic replacement
An anatomic total shoulder replacement resurfaces the joint while keeping the natural layout. A smooth metal ball goes on the arm bone, a plastic socket goes on the shoulder blade — ball where the ball was, socket where the socket was. Because it rebuilds your normal anatomy, it relies on your rotator cuff to keep the new ball centered and to move the arm. If the cuff is intact, this design tends to feel the most natural and gives the best rotation, especially the ability to reach out to the side and behind you.

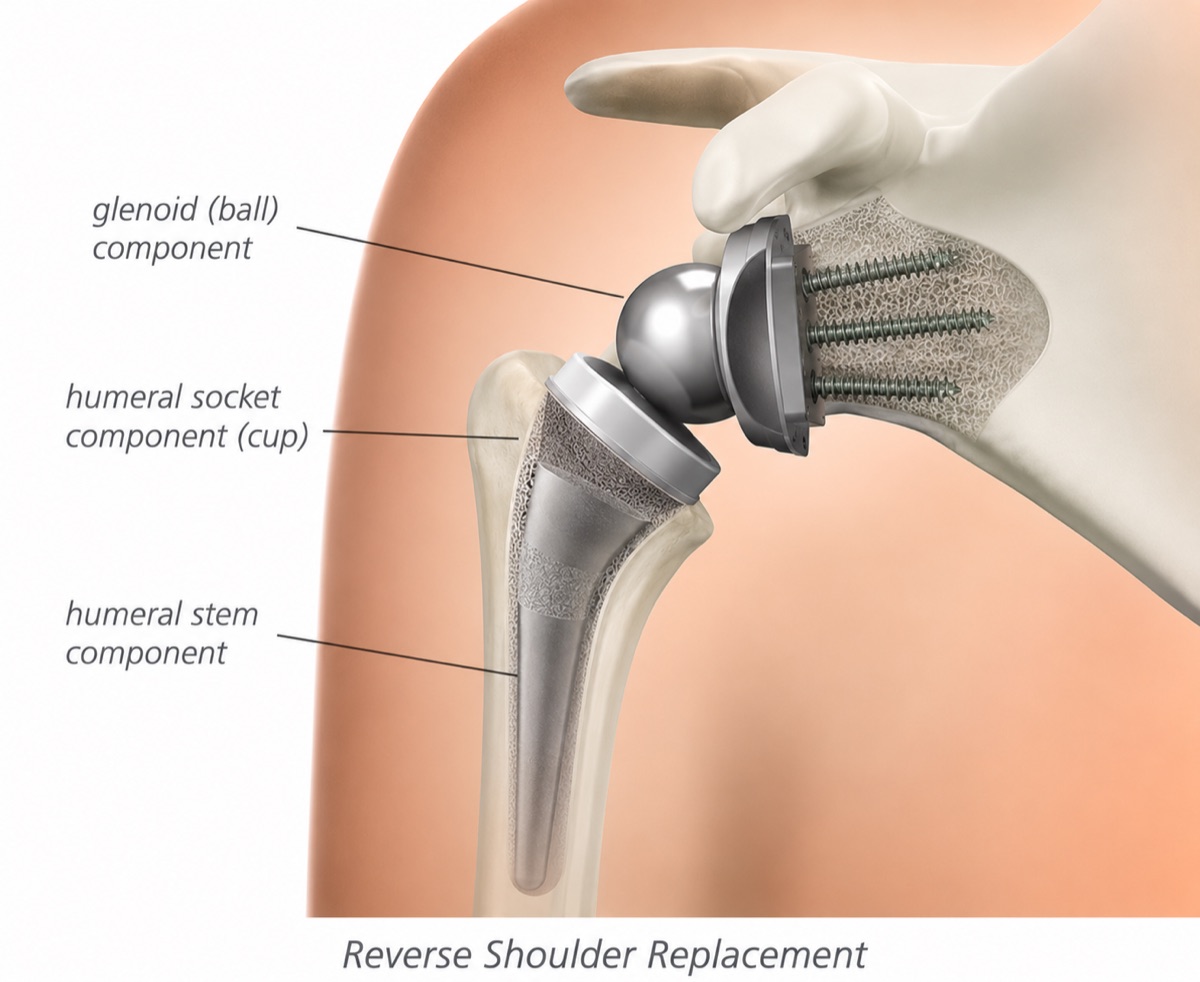
Reverse replacement
A reverse total shoulder replacement does exactly what the name says: it switches the ball and socket. The metal ball is mounted on the shoulder blade, and the cup sits on top of the arm bone. That sounds like a strange thing to do to a joint — until you realize what it accomplishes. By moving the center of rotation, the reverse design lets your deltoid (the big muscle that caps your shoulder) lift the arm directly, without needing the rotator cuff. That is why it was invented for shoulders whose cuff is torn beyond repair. It also explains its main weakness: with the geometry changed, you usually give up some external rotation — the motion you use to reach for a seatbelt or comb the back of your head.

The rotator cuff is still the dividing line
Strip away the nuance and the decision starts with one question: does your rotator cuff still work?
If the cuff is irreparably torn, or you have what we call cuff-tear arthropathy (arthritis caused by years of living with a large cuff tear), an anatomic replacement is the wrong tool. Without a functioning cuff the new ball will not stay centered, it rides upward against the socket, and the implant loosens and fails early. In that situation the reverse replacement is not a preference — it is the answer, and it is one of the more reliable operations we do.
If the cuff is fully intact and you have straightforward arthritis, an anatomic replacement has long been the default, particularly for younger, more active patients who value rotation and a natural feel.
The genuinely difficult case is the one in between: an intact cuff, but also older age, weaker tissue, or a badly worn and tilted socket (the Walch B2 and B3 glenoid patterns, where the back of the socket has eroded). This is the group where the field is actively rethinking itself — and where the recent data comes in.
What the evidence actually shows
Three threads of evidence matter here, and they point in a consistent direction.
Reverse replacements are revised less often
A 2025 systematic review and meta-analysis in Clinical Orthopaedic Surgery pooled 14 comparative studies — 4,819 shoulders, all with an intact rotator cuff — and found the revision rate was 1.7% for reverse versus 3.9% for anatomic replacements.1 The anatomic group’s failures clustered in two predictable places: loosening of the plastic glenoid socket (12.3% showed signs of it, versus essentially none of the reverse implants) and late rotator cuff failure. The reverse group had its own signature problem — scapular notching, where the implant rubs the shoulder blade (7.4%) — but that less often forced a return to the operating room.

The youngest patients carry the highest long-term risk — either way
Data from the New Zealand Joint Registry, tracking 4,346 anatomic and 7,384 reverse replacements, estimated the lifetime risk that an implant will eventually need revision.2 For patients in their late 40s that risk was roughly one in three (about 36% for anatomic, 31% for reverse), and it fell steadily with age. The message is not “reverse always wins” — it is that a replacement done at 50 has decades to potentially wear out, which is exactly why we are cautious about operating young and why durability weighs so heavily in the choice.
The function is comparable — except for rotation
Across these same analyses, patient-reported outcome scores (the standardized shoulder questionnaires, the ASES and Constant scores) and overall motion came out about the same between the two designs.13 The consistent exception is external rotation, which favored anatomic replacements by roughly 11 degrees.1 For day-to-day life that difference is often invisible; for someone who throws, swims, or reaches overhead for a living, it can matter.
Step back and the trend is unmistakable. Reverse replacements have gone from about 17% of all shoulder replacements in 2010 to roughly 43% by 2020, while the older partial replacement (hemiarthroplasty) has nearly vanished.4 Surgeons are voting with their hands, and the registry data is part of why.
What this evidence does well
- It is enormous. National joint registries follow tens of thousands of real patients across years, not a few dozen in one academic center. When a revision signal shows up across the New Zealand, UK, and Australian registries, it is hard to dismiss as a fluke.
- It uses a hard endpoint. “Did the implant have to be redone?” is far less open to interpretation than a satisfaction survey. Revision is a clear, costly event that registries capture well.
- It is consistent. Independent meta-analyses, separate registries, and a focused look at the difficult B2/B3 worn-socket shoulders all land in the same place: comparable function, lower revision with reverse.3
Where I’d pump the brakes
- Lower revision is not the same as a better shoulder. A revision counts a failure that was bad enough to reoperate. It does not capture the patient who is quietly disappointed that they can no longer rotate their arm the way they used to. Those two things can move in opposite directions, and the surveys we use are not sensitive enough to fully catch the second one.
- Follow-up is still short for a young patient’s lifetime. Reverse replacements became common only in the last 15 years. We have excellent 5- and 10-year data and very little 20- and 25-year data. A 55-year-old needs the implant to last 30 years. We are extrapolating, and we should say so plainly.
- Almost none of this is from blinded, randomized trials. These are registries and observational comparisons. Surgeons already steer sicker, older, higher-risk shoulders toward reverse replacements, which can make reverse look better — or worse — than it truly is depending on the bias. The first large randomized trial built to settle this, the UK’s RAPSODI trial, is enrolling 430 patients right now and will not report its two-year results for some time.5 Until then, every recommendation here is “the evidence suggests,” not “the evidence proves.”
- The reverse design has its own price. A large matched analysis of more than 74,000 shoulders found reverse replacements carried higher odds of certain in-hospital medical complications and short-term mechanical problems, along with longer stays — even as they reduced some other risks.6 Trading one set of risks for another is still a trade, not a free lunch.
Anatomic vs reverse shoulder replacement
Anatomic total shoulder replacement
Intact cuff, active patientRebuilds the joint the way nature laid it out — ball on the arm bone, socket on the shoulder blade. Depends on a working rotator cuff to keep the ball centered and move the arm. The traditional choice for a younger, active patient with a good cuff and decent bone in the socket.
- Most natural feel and motion when the cuff is healthy
- Better external rotation — about 11° more on average
- Preserves more of your own bone for any future surgery
- Long, mature track record
- Requires an intact, functioning rotator cuff
- Higher revision rate in pooled data (~3.9%)
- Plastic socket can loosen over time
- Vulnerable to a later rotator cuff tear
Reverse total shoulder replacement
Cuff-deficient or higher-riskSwitches the ball and socket so the deltoid muscle — not the rotator cuff — lifts the arm. Invented for shoulders with an irreparable cuff, but increasingly chosen for older patients or worn, tilted sockets even when the cuff is intact, because it is revised less often.
- Works without a functioning rotator cuff
- Lower revision rate in pooled data (~1.7%)
- Reliable for cuff-tear arthritis and worn (B2/B3) sockets
- Comparable pain relief and overall function
- Usually less external rotation
- Scapular notching (implant rubbing the blade) in some
- Removes more bone — harder to revise later
- Shorter very-long-term (20-year+) track record
How I think about the choice
When a patient sits down with an arthritic shoulder, I do not start with the implant. I start with the rotator cuff and the bone, because those two answer most of the question for us.
If the cuff is irreparable or the arthritis grew out of an old cuff tear, the conversation is short: a reverse replacement is the durable, reliable answer, and an anatomic one would be setting you up to fail. If you are younger and active with a healthy cuff, good bone, and a socket that is not badly worn, the anatomic replacement still earns its place — that extra external rotation and natural feel are real, and they matter to someone who wants their shoulder to do everything it used to.
The genuinely debatable patient is the older adult with an intact cuff but soft bone or a worn, tilted socket. A decade ago that shoulder got an anatomic replacement almost reflexively. The evidence now suggests a reverse replacement may be revised less often in exactly that setting, and I weigh that seriously. I also weigh what a patient cannot get back: a reverse replacement removes more bone, so if it ever needs redoing, the options are narrower. For an 80-year-old that rarely matters; for a 62-year-old it might.
This is also where good preoperative planning pays off. A CT-based, computer-guided plan lets us measure the socket wear precisely and place the implant to the millimeter — see how I approach that on the computer-guided shoulder replacement page. The imaging often makes a borderline decision clear.
What I will not do is tell you there is one right answer for every shoulder. The data we have is good and getting better, but the trial built to settle the hardest cases has not reported yet. Anyone who quotes you a single rule for this decision is skipping the part that actually depends on you.
The bottom line
- The rotator cuff decides most of it. A cuff that cannot be fixed points to a reverse replacement; a healthy cuff keeps anatomic on the table.
- Anatomic feels more natural and rotates better; reverse is the more forgiving, longer-lasting design when the cuff or bone is in question.
- Recent large-registry and pooled data show reverse replacements are revised less often — even in good-cuff shoulders — at the cost of some external rotation.
- Your age changes the math. The younger you are, the more a replacement’s long-term durability — and how easily it could be redone — should weigh on the choice.
- There is no universal right answer. Bring your imaging and your goals; the decision is made shoulder by shoulder, not by a rule of thumb.
If you have been told you need a shoulder replacement and you are not sure which one — or why — that is a conversation worth having with your imaging in hand. You can request a visit or call the office at (281) 690-4678.
Sources
- Thamrongskulsiri N, Limskul D, Tanpowpong T, et al. “Comparison of Revision Rates and Clinical Outcomes between Anatomic and Reverse Total Shoulder Arthroplasty for Rotator Cuff-Intact Osteoarthritis: A Systematic Review and Meta-Analysis.” Clin Orthop Surg. 2025;17(6):907–921. DOI: 10.4055/cios25012 (PMID: 41356545)
- Zhou Y, Mandaleson A, Frampton C, Hirner M. “The lifetime revision risk of primary anatomic and reverse total shoulder arthroplasty.” J Shoulder Elbow Surg. 2023;32(10):2027–2034. DOI: 10.1016/j.jse.2023.03.034 (PMID: 37178961)
- Aleisawi H, Kruse C, Nucci N, et al. “Outcomes of anatomic versus reverse shoulder arthroplasty for B2 & B3 glenoids with an intact rotator cuff: An updated systematic review and proportional meta-analysis.” Shoulder Elbow. 2025 (online). DOI: 10.1177/17585732251359590 (PMID: 40689354)
- Fornaciari P, Jamei-Martel O, Vial P. “Trends in Shoulder Arthroplasty: A Narrative Review of Predominant Indications and the Most Commonly Employed Implant Designs.” J Clin Med. 2025;14(9):3186. DOI: 10.3390/jcm14093186 (PMID: 40364217)
- Rodrick HL, Dias J, Watts AC, et al. “Anatomic versus reverse total shoulder replacement for patients with osteoarthritis and intact rotator cuff: the RAPSODI-UK randomised controlled trial protocol.” BMJ Open. 2025;15(12):e106740. DOI: 10.1136/bmjopen-2025-106740 (PMID: 41386993)
- Do DH, Thapaliya A, Sambandam S. “Reverse versus anatomic total shoulder arthroplasty: A large matched cohort analysis.” J Orthop. 2024;58:35–39. DOI: 10.1016/j.jor.2024.06.029 (PMID: 39040135)
- Atwan Y, Walton MJ, Watts AC, Trail IA. “Anatomic or reverse shoulder arthroplasty for cuff intact glenohumeral osteoarthritis.” Shoulder Elbow. 2025;17(6):697–702. DOI: 10.1177/17585732251319977 (PMID: 40093999)
This article reflects Dr. Dewan’s reading of the cited evidence at the time of publication. It is educational content, not medical advice. Your specific case may differ — schedule a consultation to discuss your imaging and history.