Meniscus tears are one of the most common knee injuries. Ask around and you will probably find a few peers or colleagues that have experienced a meniscus tear. Over the years, there has been lots of confusion about when to operate on a meniscus tear. Majority of meniscus tears do not need surgery. A good orthopedic surgeon will recommend appropriate nonoperative treatment for most meniscus tears, and understands when to recommend surgery for a meniscus tear. Below is the evidence based approach I take to treating meniscus tears.
What percentage of meniscus tears require surgery? Most do not. The majority of meniscus tears — especially the degenerative tears common after age 45 — improve with non-operative care, and only a minority ever need an operation. Is arthroscopy necessary for a meniscus tear? Usually not as a first step. For degenerative tears, high-quality evidence (including the 10-year FIDELITY trial on arthroscopy for degenerative meniscus tears) shows surgery is no better than structured physical therapy, so I reserve arthroscopy for acute tears in younger, active knees or for tears that are truly locking or catching the joint.
What is the meniscus?
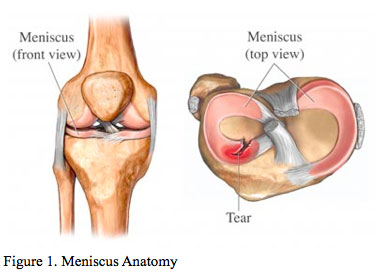
(picture courtesy of http://ortho.ucla.edu/)
The meniscus is a wedge-like cushion made of cartilage that is sandwiched between the thigh bone and shin bone at the knee joint. The blood supply of the meniscus is limited to only the outermost portion. The central portion lacks any blood supply. The contour of the meniscus matches the end of the thigh bone. Consequently, the meniscus helps maximize contact surface area of the thigh bone with the shin bone. When the meniscus is disrupted/damaged it affects its ability to distribute the pressure exerted by the thigh bone evenly over the top of the shin bone. As a result forces can become excessively concentrated in certain parts of the knee producing symptoms and potentially accelerating the wear and tear of the joint. Once a meniscus is torn, loose fragments can shift around in the knee, interfering with knee joint motion. This can sometimes produce sensations of locking, clicking, or catching inside the knee.
What is a medial meniscus tear? The knee has two menisci: the medial meniscus on the inner side of the knee and the lateral meniscus on the outer side. A medial meniscus tear is a tear of that inner cushion — the most common location for a meniscus tear — and it typically causes pain along the inside of the knee, sometimes with clicking, catching, or a pinch when you squat or twist.
I often tell patients, having a torn meniscus is akin to having a pebble in your shoe. Sometimes, the “pebble” or meniscal fragment can get incarcerated or trapped between the thigh bone and shin bone interfering with smooth joint motion and produce a sharp pinching type pain. Other times, the “pebble” or meniscal fragment shifts back to where it belongs and does not interfere with smooth knee motion, making it much less symptomatic.
How often this “pebble” gets in the way often dictates how aggressive the treatment that is pursued.
How do you diagnose a meniscus tear?
The evaluation for acute meniscus tears begins with a thorough history and clinical exam. There are several provocative clinical tests that attempt to elicit pain from a torn meniscus. My goto favorites are the McMurray test, Flexion Circumduction test, and Thessaly test. X-rays are usually then obtained to help establish if there are any predisposing anatomical risk factors related to knee alignment and to confirm if there are any underlying signs of arthritis in the knee. At this point, based on the history, physical, and imaging findings, I make a distinction between suspected meniscus tears that are chronic and degenerative and those that are acute and traumatic. It is important to distinguish the type of meniscus tear to best guide the treatment. If the X-ray does not show any arthritis, and there is a high suspicion for an acute type meniscus tear (see below), MRI can be obtained to evaluate the meniscus and other soft tissues. When knee arthritis is present an MRI is not necessary initially since the treatment for a more indolent, chronic, degenerative meniscus tear always begins with less risky non-operative options (see below). With the latter, if the non operative treatment ultimately fails, then an MRI may be warranted to investigate further.
Chronic degenerative meniscus tears
Chronic and degenerative meniscus tears are secondary to joint wear and degeneration. Degenerative meniscus tears are in fact very common. Once there is evidence of arthritis in the knee, more than 60% of patients will show evidence of meniscus tearing on an MRI, irrespective of whether they report knee pain or not. As the knee joint accumulates wear and tear, it is expected that the meniscus will also exhibit evidence of wear and tear such as meniscus tears. The quality of the cartilage that composes the meniscus degenerates as the knee is subject to more wear and tear. As a physician, the challenge is determining whether new symptoms experienced at the knee are secondary to osteoarthritis progression or from a new meniscus tear. To this end, in some circumstances an MRI to evaluate the knee is warranted.
Treating meniscus tears in a degenerative knee has gotten significant attention lately both in the lay press (see New York Times article here) and in the medical literature (see article here). For many years, orthopedic surgeons had been recommending arthroscopic surgery to debride meniscus tears seen on MRI in painful knees. Many however began to note that patients were not improving over time in spite of surgery. This observation was confirmed in studies, including a publicized trial in the New England Journal of Medicine. The take home message of this study and other subsequent ones is that surgery should never be the first choice in the setting of a degenerative meniscus tear.
For new onset knee pain in a degenerative knee in someone over the age of 45, even in the setting of MRI evidence of a meniscal tear, my first treatment recommendations include activity modification, physical therapy, weight loss if obese, anti-inflammatories, and an adjunct steroid injection in the right circumstances.
Activity Modification. Certain activities place more demand on the knee than others. High impact sports like running for example, can be very harsh on knees, and provoke more inflammation and irritation. There are other low impact activities that are gentler on sore knees with degenerative changes. Swimming or water aerobics are perhaps the best activities since the buoyancy achieved in water eliminates a significant amount of force transmission across the knees. Rowing and biking are another two great activities to maintain physical fitness in the setting of degenerative meniscus tears. In these two activities, by assuming a seated position, there is less weight transmission through the knees. Not as gentle as rowing and swimming, but still better than running, an elliptical exercise machine is another way of reducing the force of impact across the knees. The theme here is modifying activities to ones that spare the knees.
Physical Therapy. The rationale for physical therapy is often questioned by patients. The purpose of physical therapy is to strengthen the muscles surrounding the knee. Stronger muscles dampen the forces across the knee joint and in turn can often alleviate the symptoms of a degenerative knee. Many people don’t realize how quickly their knee can weaken while coping with knee pain. Even after just a week of favoring the knee, muscle atrophy can begin to develop. If the process has been ongoing for months, many times the subtle gradual loss in strength around the knee might not be perceived by the patient as they compensate by placing more stress on the neighboring hip or ankle.
Weight Loss. Weight loss can go a long ways toward alleviating symptoms in a degenerative knee. Due to the physics and forces across the knee during the gait cycle, there can be times depending on the activity one is doing when forces across the knee can exceed 9 times body weight. With that kind of multiplier, you can see how even loosing 10 pounds of weight can make your knees feel effectively 90 pounds lighter! That often is enough to make insufferable knee pain into something a bit more manageable.
Anti-inflammatories. Is meloxicam good for a torn meniscus? Yes — meloxicam is one of the anti-inflammatories I commonly recommend for a symptomatic meniscus tear. It is a once-daily NSAID that reduces the inflammation driving the pain, though it treats symptoms rather than healing the tear. This class of drugs (referred to as non-steroidal anti-inflammatory drugs or NSAIDs), can help manage the symptoms from a degenerative meniscal tear. While the analgesic affect of these drugs maybe immediate, I often counsel patients they need to take it for a sustained period (2-3 weeks) to realize the anti-inflammatory benefits. As long as there are no health concerns such as drug allergy, kidney problems, or drug interactions, I recommend patients try a course of Meloxicam, Ibuprofen, or Naproxen to see if it helps manage their symptoms.
Steroid injections. The knee joint is enclosed in a capsule like balloon structure where joint fluid is contained. If all else fails, and there is already signs of degeneration from arthritis in the knee, I then propose a steroid injection to help “put the fire out” or stem the inflammation in the knee. While not every patient responds to steroid injections, a significant number can get anywhere from 3-6 months relief of their pain after the injection. If the pain has not improved with any of the above steps, then this may be an option worth considering.
Finally if all the measures above fail, in refractory cases where the pain is still unbearable, and when the clinical exam is consistent with a symptomatic degenerative meniscus tear, I offer arthroscopic surgery. Arthroscopic knee surgery is discussed in detail below, but the goal of surgery is to “trim” the torn portion of the meniscus that may be generating their symptoms.
Acute traumatic meniscus tears
Athletes, particularly those that play contact sports, are susceptible to acute and traumatic meniscus injury. Acute traumatic tears can also occur after a sudden movement or change in position. The nature and behavior of acute meniscus tears, especially in the absence of underlying osteoarthritis in an active individual, is very different than the chronic degenerative meniscus tears described above. These tears are not nearly as common as the degenerative tears discussed above, and are usually secondary to large forces sustained across the meniscal tissue as opposed to chronic breakdown of meniscal cartilage. In younger patients, where the meniscal cartilage is robust, and unlikely to have changes secondary to tissue deterioration, the primary goal is to preserve and repair as much tissue as possible to mitigate the risks associated with the loss of the meniscus tissue and its role in shock absorption and load distribution at the knee. In younger patients with symptomatic tears that are producing symptoms such as catching or locking of the knee, or with persistent pain from the meniscus that interferes with their activities that cannot be managed with anti-inflammatories, I recommend arthroscopic surgery — ideally a repair that preserves the meniscus. See a step-by-step walkthrough of a real arthroscopic bucket-handle meniscus repair for what that looks like.
Arthroscopic meniscus surgery

Arthroscopic surgery of the knee is one of the most common surgeries performed in the United States. The procedure involves inserting a camera about the size of a pen into the knee joint. From another 1 cm incision around the knee, I insert specialized arthroscopic tools to manipulate structures inside the knee. In older patients, with chronic degenerative tears, as described above, surgery is the last resort. In contrast, for younger patients, with no signs of pre-existing knee arthritis, arthroscopic surgery is considered.
During arthroscopic surgery the first and foremost goal is to attempt a meniscal repair. When the tear is in the outermost zone with potential for healing (often the younger patients with acute tears), I use arthroscopic sutures to stitch the torn meniscus. For young, non-smokers, with tears in the outermost portion of their meniscus, the potential for meniscal healing/repair is higher. The blood supply which provides the nutrients and components necessary for a healing response are only found in the outermost portion of the meniscus. Studies have shown >85% of patients that underwent repair report good-excellent outcomes. In contrast, degenerative tears of the meniscus reflect a break down in the underlying meniscus structure and do not improve with repair.
If the meniscus tissue is damaged beyond repair (often the case in chronic degenerative tears), or the tear is in the central portion that has no healing potential, then I use arthroscopic tools to remove or “trim” the damaged, non-functioning, part of the meniscus. Arthroscopic meniscus trimming, otherwise known as partial menisectomy, has a reported success rate of >80% in patients that have failed non operative therapy, particularly in the setting of mechanical symptoms and minimal pre-existing arthritis. With underlying arthritis and degenerative knee changes, the result is less predictable. Therefore, for degenerative chronic type tears, surgery is reserved as a last resort. The hard part is often convincing patients that the arthroscopic surgery is not a quick fix in the setting of chronic degenerative meniscus tears. While there are circumstances where arthroscopic surgery produces an excellent and predictable outcome, with degenerative meniscus tears in the presence of osteoarthritis, the pain relief can be variable from surgery.
Learn more about the arthroscopic knee surgery I perform, or if your injury also involved a pop and instability, read about ACL reconstruction surgery. Call 281-690-4678 now to schedule a consultation to discuss your knee problem.
Sources:
http://www.nytimes.com/2016/08/04/upshot/the-right-to-know-that-an-operation-is-next-to-useless.html?_r=0
http://www.ncbi.nlm.nih.gov/pubmed/25157057
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2897006/
http://www.nejm.org/doi/full/10.1056/NEJMoa1301408
http://orthoinfo.aaos.org/topic.cfm?topic=A00358